

The Safety and Outcome of Minimally Invasive Staged Segmental Artery Coil Embolization (MIS2ACE) Prior Thoracoabdominal Aortic Aneurysm Repair: A Single-Center Study, Systematic Review, and Meta-Analysis
- PMID: 38592242
- PMCID: PMC10934631
- DOI: 10.3390/jcm13051408
The Safety and Outcome of Minimally Invasive Staged Segmental Artery Coil Embolization (MIS2ACE) Prior Thoracoabdominal Aortic Aneurysm Repair: A Single-Center Study, Systematic Review, and Meta-Analysis
Abstract
Background: Minimally Invasive Staged Segmental Artery Coil Embolization (MIS2ACE) is a novel technique of spinal cord preconditioning used to reduce the risk of paraplegia in thoracoabdominal aortic aneurysm (TAAA) repair. In this study, we report our experience with MIS2ACE, including both degenerative and post-dissection TAAA, while we attempt to systematically summarize relevant data available in the literature.
Design: single-center observational study with systematic review of the literature and meta-analysis.
Methods: Initial retrospective analysis of 7 patients undergoing MIS2ACE over 12 sessions with a subsequent systematic review of the literature and meta-analysis of the available published data (PROSPERO protocol number: CRD42023477411). Baseline patient and aneurysm characteristics, along with procedural technique and outcomes, were analyzed. One-arm pooling of proportions was used to summarize available published data.
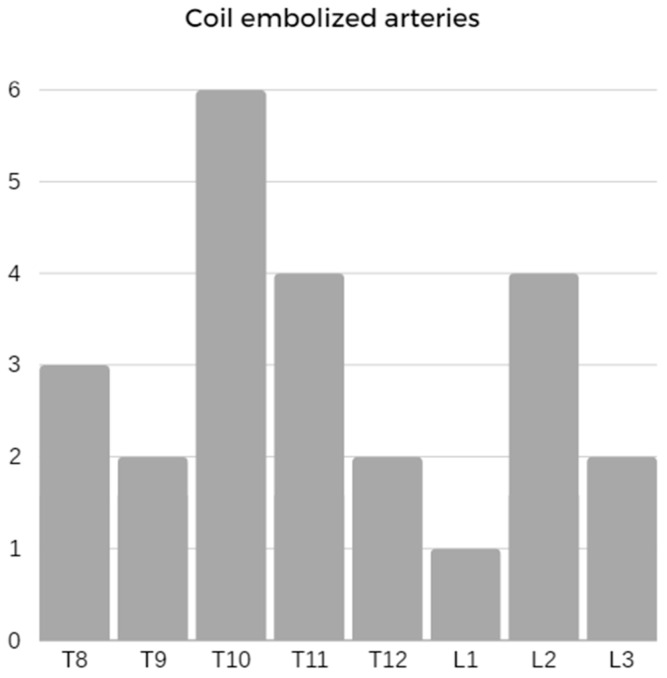
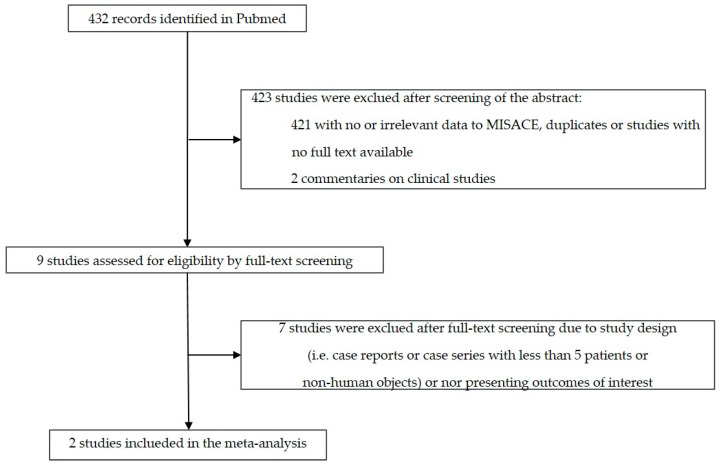
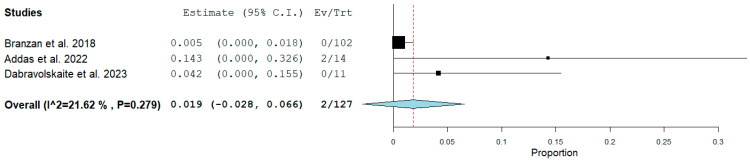
Results: We treated seven patients (5 males, 71%) with a median age of 69 years (IQR 55,69). According to the Crawford classification, five patients (1%) had extent II TAAA, and two (29%) had extent III TAAA. Five patients (71%) had post-dissection -TAAA; four of them were after Stanford type A dissection, and one had a chronic type B dissection. Three patients (43%) had connective tissue disease. Of the seven patients, six (86%) underwent previous aortic surgery, while the median aneurysm diameter was 58 mm (IQR 55,58). MIS2ACE was successful in 11 sessions (92%). The median number of embolized arteries was 4 (IQR 1,4). There were no periprocedural complications in any embolization. The median embolization-operation time interval was 37.0 days (IQR 31,78). Two patients had open and five endovascular treatment. There were no events of spinal cord ischemia either after MIS2ACE or after the aortic repair. Out of the 432 initially retrieved articles, we included two studies in the meta-analysis, including patients with MIS2ACE for spinal cord preconditioning in addition to our cohort. The prevalence of pooled postoperative spinal cord ischemia among MIS2ACE patients is 1.9% (95% CI -0.028 to 0.066, p = 0.279; 3 studies; 81 patients, 127 coiling sessions).
Conclusions: While the current published data is limited, our study further confirms that MIS2ACE is a technically feasible and safe option for spinal cord preconditioning.
Keywords: coil embolization; segmental artery; thoraco-abdominal aortic aneurysm repair.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Minimally Invasive Segmental Artery Coil Embolization (MISACE) Prior to Endovascular Thoracoabdominal Aortic Aneurysm Repair.Cardiovasc Intervent Radiol. 2022 Oct;45(10):1462-1469. doi: 10.1007/s00270-022-03230-y. Epub 2022 Aug 4. Cardiovasc Intervent Radiol. 2022. PMID: 35927497
-
Minimally invasive staged segmental artery coil embolization (MIS2ACE) for spinal cord protection.Ann Cardiothorac Surg. 2023 Sep 28;12(5):492-499. doi: 10.21037/acs-2023-scp-21. Epub 2023 Sep 19. Ann Cardiothorac Surg. 2023. PMID: 37817850 Free PMC article.
-
First-in-man endovascular preconditioning of the paraspinal collateral network by segmental artery coil embolization to prevent ischemic spinal cord injury.J Thorac Cardiovasc Surg. 2015 Apr;149(4):1074-9. doi: 10.1016/j.jtcvs.2014.12.025. Epub 2014 Dec 18. J Thorac Cardiovasc Surg. 2015. PMID: 25906717
-
Safety and Efficacy of Intentional Celiac Artery Coverage in Endovascular Management of Thoracoabdominal Aortic Diseases: A Systematic Review and Meta-analysis.J Endovasc Ther. 2022 Aug;29(4):646-658. doi: 10.1177/15266028211059451. Epub 2021 Nov 26. J Endovasc Ther. 2022. PMID: 34836463
-
Spinal cord ischemia in open and endovascular thoracoabdominal aortic aneurysm repair: new concepts.J Cardiovasc Surg (Torino). 2014 Apr;55(2 Suppl 1):159-68. J Cardiovasc Surg (Torino). 2014. PMID: 24796909 Review.
References
-
- Dias-Neto M., Tenorio E.R., Huang Y., Jakimowicz T., Mendes B.C., Kölbel T., Sobocinski J., Bertoglio L., Mees B., Gargiulo M., et al. Comparison of single- and multistage strategies during fenestrated-branched endovascular aortic repair of thoracoabdominal aortic aneurysms. J. Vasc. Surg. 2023;77:1588–1597.e4. doi: 10.1016/j.jvs.2023.01.188. - DOI - PubMed
-
- Branzan D., Etz C.D., Moche M., Von Aspern K., Staab H., Fuchs J., Bergh F.T., Scheinert D., Schmidt A. Ischaemic preconditioning of the spinal cord to prevent spinal cord ischaemia during endovascular repair of thoracoabdominal aortic aneurysm: First clinical experience. EuroIntervention. 2018;14:828–835. doi: 10.4244/EIJ-D-18-00200. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
