

Clinical Outcomes in Children With Human Immunodeficiency Virus Treated for Nonsevere Tuberculosis in the SHINE Trial
- PMID: 38592950
- PMCID: PMC11259218
- DOI: 10.1093/cid/ciae193
Clinical Outcomes in Children With Human Immunodeficiency Virus Treated for Nonsevere Tuberculosis in the SHINE Trial
Abstract
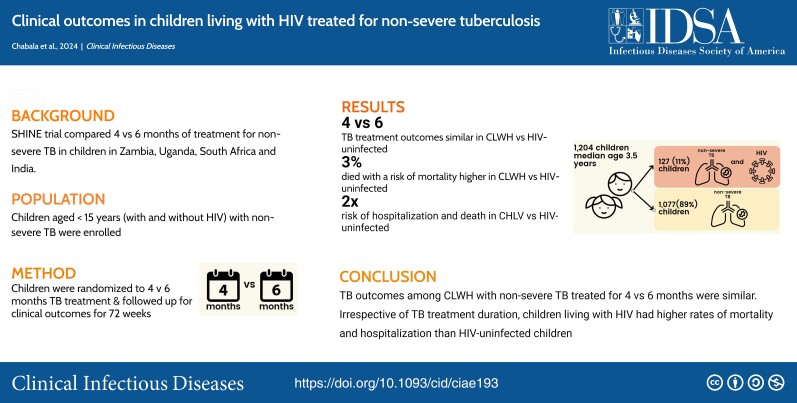
Background: Children with human immunodeficiency virus (HIV, CWH) are at high risk of tuberculosis (TB) and face poor outcomes, despite antiretroviral therapy (ART). We evaluated outcomes in CWH and children not living with HIV treated for nonsevere TB in the SHINE trial.
Methods: SHINE was a randomized trial that enrolled children aged <16 years with smear-negative, nonsevere TB who were randomized to receive 4 versus 6 months of TB treatment and followed for 72 weeks. We assessed TB relapse/recurrence, mortality, hospitalizations, grade ≥3 adverse events by HIV status, and HIV virological suppression in CWH.
Results: Of 1204 children enrolled, 127 (11%) were CWH, of similar age (median, 3.6 years; interquartile range, 1.2, 10.3 versus 3.5 years; 1.5, 6.9; P = .07) but more underweight (weight-for-age z score, -2.3; (3.3, -0.8 versus -1.0; -1.8, -0.2; P < .01) and anemic (hemoglobin, 9.5 g/dL; 8.7, 10.9 versus 11.5 g/dL; 10.4, 12.3; P < .01) compared with children without HIV. A total of 68 (54%) CWH were ART-naive; baseline median CD4 count was 719 cells/mm3 (241-1134), and CD4% was 16% (10-26). CWH were more likely to be hospitalized (adjusted odds ratio, 2.4; 1.3-4.6) and to die (adjusted hazard ratio [aHR], 2.6; 95% confidence interval [CI], 1.2 to 5.8). HIV status, age <3 years (aHR, 6.3; 1.5, 27.3), malnutrition (aHR, 6.2; 2.4, 15.9), and hemoglobin <7 g/dL (aHR, 3.8; 1.3,11.5) independently predicted mortality. Among children with available viral load (VL), 45% and 61% CWH had VL <1000 copies/mL at weeks 24 and 48, respectively. There was no difference in the effect of randomized treatment duration (4 versus 6 months) on TB treatment outcomes by HIV status (P for interaction = 0.42).
Conclusions: We found no evidence of a difference in TB outcomes between 4 and 6 months of treatment for CWH treated for nonsevere TB. Irrespective of TB treatment duration, CWH had higher rates of mortality and hospitalization than their counterparts without HIV. Clinical Trials Registration. ISRCTN63579542.
Keywords: adverse events; children with HIV; mortality; tuberculosis; viral suppression.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. C. C., E. W., S. H., Vi. M., and A. C. H. report institutional funding to participate as SHINE trial sites from the UK MRC–Clinical Trials at University College, London, through a prime grant award from UK MRC, Wellcome Trust, and Department for International Development (grant MR/L004445/1). A. T., A. K., and D. G. report a COVID 19 Grant Extension Allocation award 181573 from UK Research Innovation. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization . Global tuberculosis report 2023. Geneva, Switzerland: World Health Organization, 2023.
-
- UNAIDS . UNAIDS data 2022. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS, 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
