

Somatic mutations in FAS pathway increase hemophagocytic lymphohistiocytosis risk in patients with T- and/or NK-cell lymphoma
- PMID: 38593227
- PMCID: PMC11222957
- DOI: 10.1182/bloodadvances.2023011733
Somatic mutations in FAS pathway increase hemophagocytic lymphohistiocytosis risk in patients with T- and/or NK-cell lymphoma
Abstract
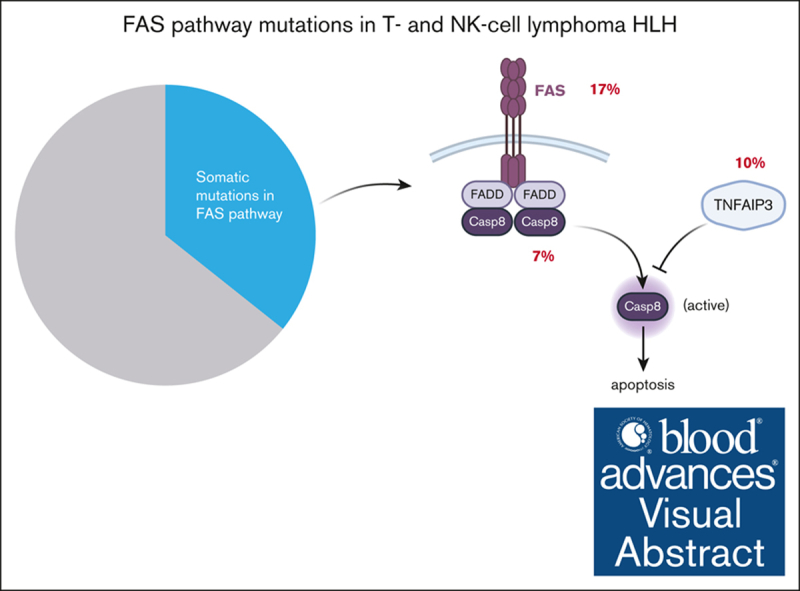
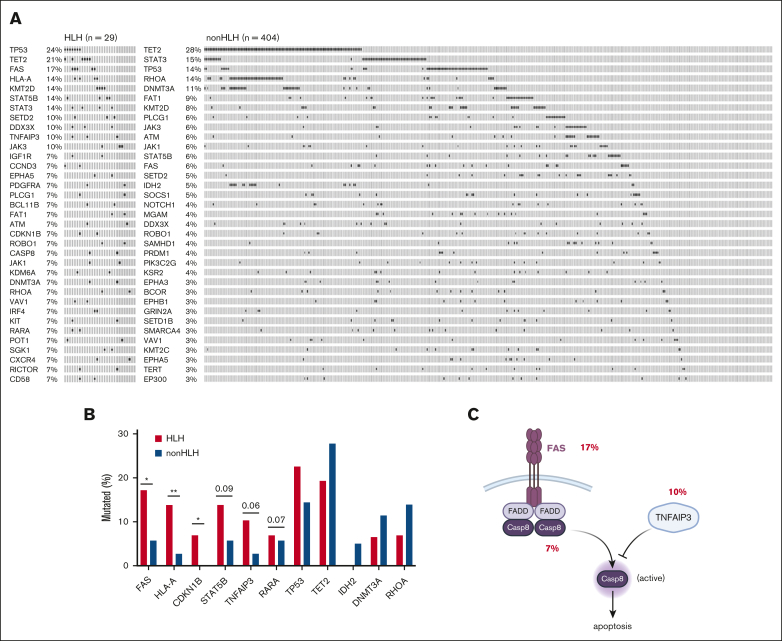
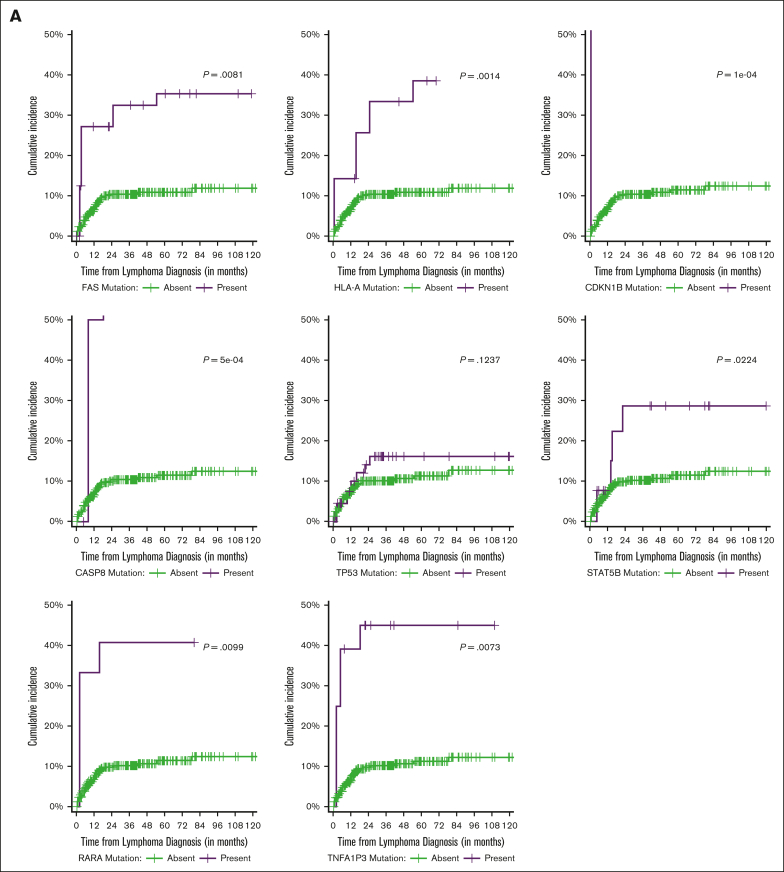
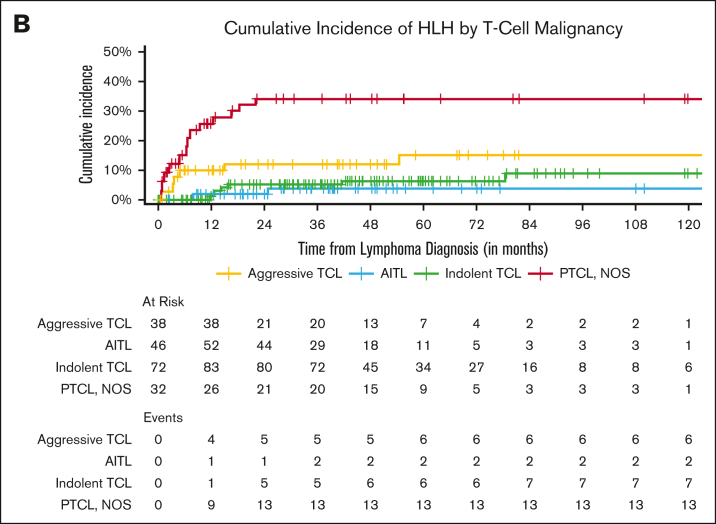
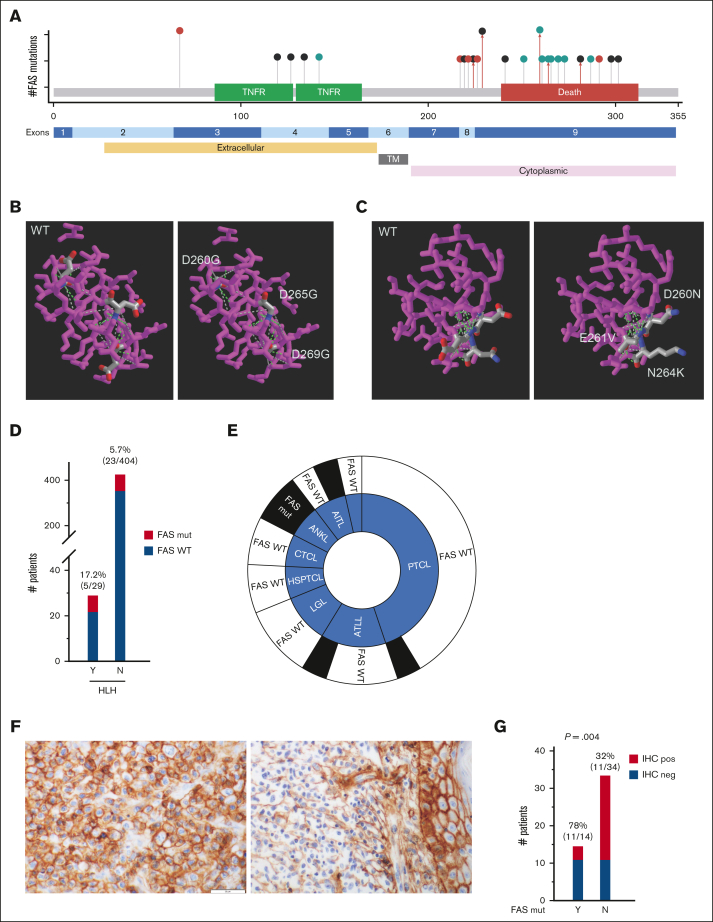
Although significant progress has been made in understanding the genetic basis of primary hemophagocytic lymphohistiocytosis (HLH), the pathogenesis of secondary HLH, the more prevalent form, remains unclear. Among the various conditions giving rise to secondary HLH, HLH in patients with lymphoma (HLH-L) accounts for a substantial proportion. In this study, we investigated the role of somatic mutations in the pathogenesis of HLH-L in a cohort of patients with T- and/or natural killer-cell lymphoma. We identified a 3-time higher frequency of mutations in FAS pathway in patients with HLH-L. Patients harboring these mutations had a 5-time increased HLH-L risk. These mutations were independently associated with inferior outcome. Hence, our study demonstrates the association between somatic mutations in FAS pathway and HLH-L. Further studies are warranted on the mechanistic role of these mutations in HLH-L.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: W.T.J. received consulting fees from Myeloid Therapeutics. S.V. served on the advisory board for Immunai and received consulting fees from ADC Therapeutics and Koch Disruptive Technologies. S.M.H. received research funding from ADC Therapeutics, Affimed, Aileron, Celgene, CRISPR Therapeutics, Daiichi Sankyo, Forty Seven Inc, Kyowa Hakko Kirin, Millennium/Takeda, Seattle Genetics, Trillium Therapeutics, and Verastem/SecuraBio, and consulting fees from Acrotech Biopharma, ADC Therapeutics, Astex, Auxilus Pharma, Merck, C4 Therapeutics, Celgene, Cimieo Therapeutics, Daiichi Sankyo, Janssen, Kura Oncology, Kyowa Hakko Kirin, Myeloid Therapeutics, ONO Pharmaceuticals, Seattle Genetics, SecuraBio, Shoreline Biosciences Inc, Takeda, Trillium Therapeutics, Tubulis, Verastem/SecuraBio, Vividion Therapeutics, and Yingli Pharma Ltd. A. Dogan served as a consultant for Incyte, EUSA Pharma, and Loxo, and receives research support from Roche and Takeda. W.X. received research support from Stemline Therapeutics. The remaining authors declare no competing financial interests.
The current affiliation for R.S. is Sardana Labs, Punjab, India.
Figures
References
-
- Al-Samkari H, Berliner N. Hemophagocytic lymphohistiocytosis. Annu Rev Pathol. 2018;13(1):27–49. - PubMed
-
- La Rosée P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465–2477. - PubMed
-
- Han AR, Lee HR, Park B-B, et al. Lymphoma-associated hemophagocytic syndrome: clinical features and treatment outcome. Ann Hematol. 2007;86(7):493–498. - PubMed
-
- Sano H, Kobayashi R, Tanaka J, et al. Risk factor analysis of non-Hodgkin lymphoma-associated hemophagocytic syndromes: a multicenter study. Br J Haematol. 2014;165(6):786–792. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
