

Use of menopausal hormone therapy beyond age 65 years and its effects on women's health outcomes by types, routes, and doses
- PMID: 38595196
- PMCID: PMC11465799
- DOI: 10.1097/GME.0000000000002335
Use of menopausal hormone therapy beyond age 65 years and its effects on women's health outcomes by types, routes, and doses
Abstract
Objectives: The study aims to assess the use of menopausal hormone therapy beyond age 65 years and its health implications by types of estrogen/progestogen, routes of administration, and dose strengths.
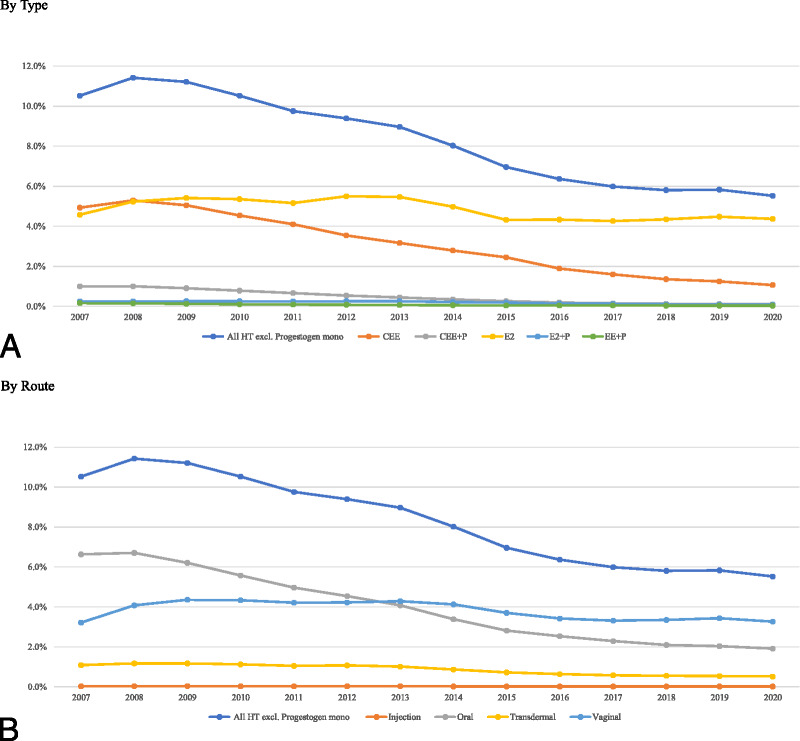
Methods: Using prescription drug and encounter records of 10 million senior Medicare women from 2007-2020 and Cox regression analyses adjusted for time-varying characteristics of the women, we examined the effects of different preparations of menopausal hormone therapy on all-cause mortality, five cancers, six cardiovascular diseases, and dementia.
Results: Compared with never use or discontinuation of menopausal hormone therapy after age 65 years, the use of estrogen monotherapy beyond age 65 years was associated with significant risk reductions in mortality (19% or adjusted hazards ratio, 0.81; 95% CI, 0.79-0.82), breast cancer (16%), lung cancer (13%), colorectal cancer (12%), congestive heart failure (CHF) (5%), venous thromboembolism (3%), atrial fibrillation (4%), acute myocardial infarction (11%), and dementia (2%). For the use of estrogen and progestogen combo-therapy, both E+ progestin and E+ progesterone were associated with increased risk of breast cancer by 10%-19%, but such risk can be mitigated using low dose of transdermal or vaginal E+ progestin. Moreover, E+ progestin exhibited significant risk reductions in endometrial cancer (45% or adjusted hazards ratio, 0.55; 95% CI, 0.50-0.60), ovarian cancer (21%), ischemic heart disease (5%), CHF (5%), and venous thromboembolism (5%), whereas E+ progesterone exhibited risk reduction only in CHF (4%).
Conclusions: Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with E2 rather than conjugated estrogen.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The Menopause Society.
Conflict of interest statement
Financial disclosures/conflicts of interest: None reported.
Figures
References
-
- Rossouw JE Anderson GL Prentice RL, et al.; Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA J Am Med Assoc 2002;288:321–333. doi: 10.1001/jama.288.3.321 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
