

Surgical intervention combined with weight-bearing walking training promotes recovery in patients with chronic spinal cord injury: a randomized controlled study
- PMID: 38595294
- PMCID: PMC11168509
- DOI: 10.4103/NRR.NRR-D-23-01198
Surgical intervention combined with weight-bearing walking training promotes recovery in patients with chronic spinal cord injury: a randomized controlled study
Abstract
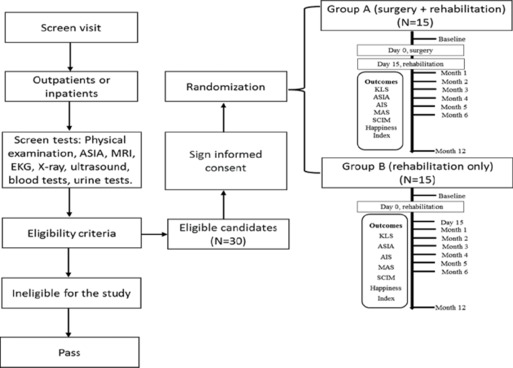
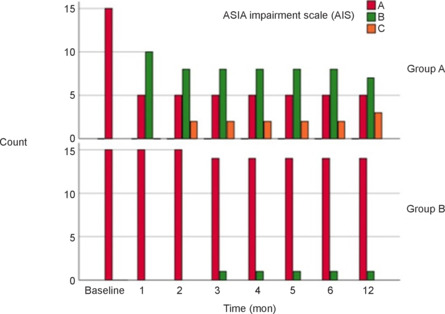
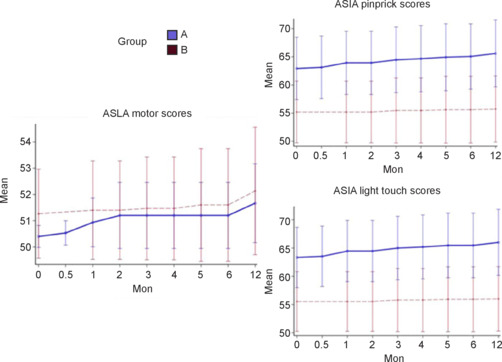
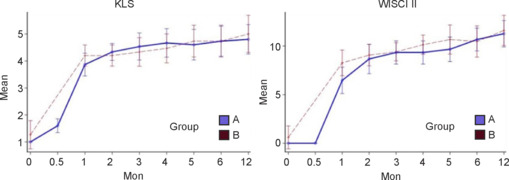
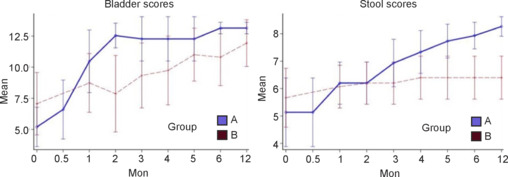
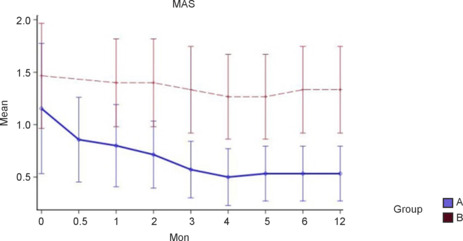
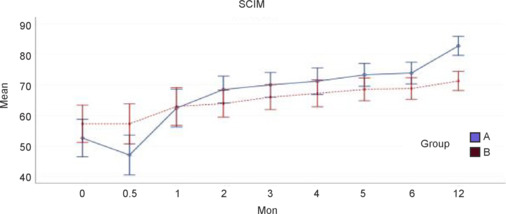
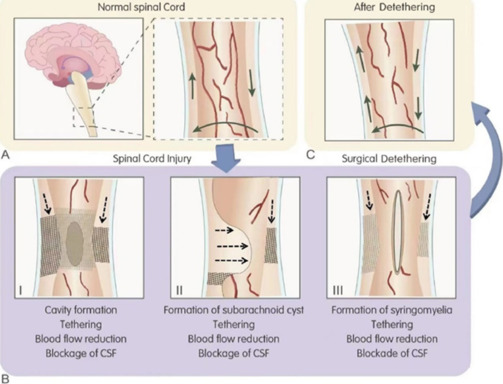
JOURNAL/nrgr/04.03/01300535-202412000-00032/figure1/v/2024-04-08T165401Z/r/image-tiff For patients with chronic spinal cord injury, the conventional treatment is rehabilitation and treatment of spinal cord injury complications such as urinary tract infection, pressure sores, osteoporosis, and deep vein thrombosis. Surgery is rarely performed on spinal cord injury in the chronic phase, and few treatments have been proven effective in chronic spinal cord injury patients. Development of effective therapies for chronic spinal cord injury patients is needed. We conducted a randomized controlled clinical trial in patients with chronic complete thoracic spinal cord injury to compare intensive rehabilitation (weight-bearing walking training) alone with surgical intervention plus intensive rehabilitation. This clinical trial was registered at ClinicalTrials.gov (NCT02663310). The goal of surgical intervention was spinal cord detethering, restoration of cerebrospinal fluid flow, and elimination of residual spinal cord compression. We found that surgical intervention plus weight-bearing walking training was associated with a higher incidence of American Spinal Injury Association Impairment Scale improvement, reduced spasticity, and more rapid bowel and bladder functional recovery than weight-bearing walking training alone. Overall, the surgical procedures and intensive rehabilitation were safe. American Spinal Injury Association Impairment Scale improvement was more common in T7-T11 injuries than in T2-T6 injuries. Surgery combined with rehabilitation appears to have a role in treatment of chronic spinal cord injury patients.
Copyright © 2024 Copyright: © 2024 Neural Regeneration Research.
Conflict of interest statement
Figures
Similar articles
-
Surgical intervention combined with weight-bearing walking training improves neurological recoveries in 320 patients with clinically complete spinal cord injury: a prospective self-controlled study.Neural Regen Res. 2021 May;16(5):820-829. doi: 10.4103/1673-5374.297080. Neural Regen Res. 2021. PMID: 33229715 Free PMC article.
-
Against the odds: what to expect in rehabilitation of chronic spinal cord injury with a neurologically controlled Hybrid Assistive Limb exoskeleton. A subgroup analysis of 55 patients according to age and lesion level.Neurosurg Focus. 2017 May;42(5):E15. doi: 10.3171/2017.2.FOCUS171. Neurosurg Focus. 2017. PMID: 28463613
-
Recovery of Volitional Motor Control and Overground Walking in Participants With Chronic Clinically Motor Complete Spinal Cord Injury: Restoration of Rehabilitative Function With Epidural Spinal Stimulation (RESTORES) Trial-A Preliminary Study.J Neurotrauma. 2024 May;41(9-10):1146-1162. doi: 10.1089/neu.2023.0265. Epub 2024 Jan 5. J Neurotrauma. 2024. PMID: 38115642 Clinical Trial.
-
Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury.J Neurol Phys Ther. 2020 Jan;44(1):49-100. doi: 10.1097/NPT.0000000000000303. J Neurol Phys Ther. 2020. PMID: 31834165 Review.
-
Effectiveness of robotic-assisted gait training on cardiopulmonary fitness and exercise capacity for incomplete spinal cord injury: A systematic review and meta-analysis of randomized controlled trials.Clin Rehabil. 2023 Mar;37(3):312-329. doi: 10.1177/02692155221133474. Epub 2022 Nov 14. Clin Rehabil. 2023. PMID: 36373899
Cited by
-
Passive activity enhances residual control ability in patients with complete spinal cord injury.Neural Regen Res. 2025 Aug 1;20(8):2337-2347. doi: 10.4103/NRR.NRR-D-23-01812. Epub 2024 May 13. Neural Regen Res. 2025. PMID: 39359092 Free PMC article.
-
Multi-target neural circuit reconstruction and enhancement in spinal cord injury.Neural Regen Res. 2026 Mar 1;21(3):957-971. doi: 10.4103/NRR.NRR-D-24-00434. Epub 2025 Jan 29. Neural Regen Res. 2026. PMID: 39885668 Free PMC article.
References
-
- Akpinar P, Atici A, Ozkan FU, Aktas I, Kulcu DG, Sarı A, Durmus B. Reliability of the Modified Ashworth Scale and Modified Tardieu Scale in patients with spinal cord injuries. Spinal Cord. 2017;55:944–949. - PubMed
-
- Alexander JK, Popovich PG. Neuroinflammation in spinal cord injury: Therapeutic targets for neuroprotection and regeneration. Prog Brain Res. 2009;175:125–137. - PubMed
-
- Anderson KD, Acuff ME, Arp BG, Backus D, Chun S, Fisher K, Fjerstad JE, Graves DE, Greenwald K, Groah SL, Harkema SJ, Horton JA, 3rd, Huang MN, Jennings M, Kelley KS, Kessler SM, Kirshblum S, Koltenuk S, Linke M, Ljungberg I, et al. United States (US) multi-center study to assess the validity and reliability of the Spinal Cord Independence Measure (SCIM III) Spinal Cord. 2011;49:880–885. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
