

Association of metabolic syndrome and sarcopenia with all-cause and cardiovascular mortality: a prospective cohort study based on the NHANES
- PMID: 38596221
- PMCID: PMC11002088
- DOI: 10.3389/fendo.2024.1346669
Association of metabolic syndrome and sarcopenia with all-cause and cardiovascular mortality: a prospective cohort study based on the NHANES
Abstract
Background: Metabolic syndrome (MetS) and sarcopenia (SP) have emerged as significant public health concerns in contemporary societies, characterized by shared pathophysiological mechanisms and interrelatedness, leading to profound health implications. In this prospective cohort study conducted within a US population, we aimed to examine the influence of MetS and SP on all-cause and cardiovascular mortality.
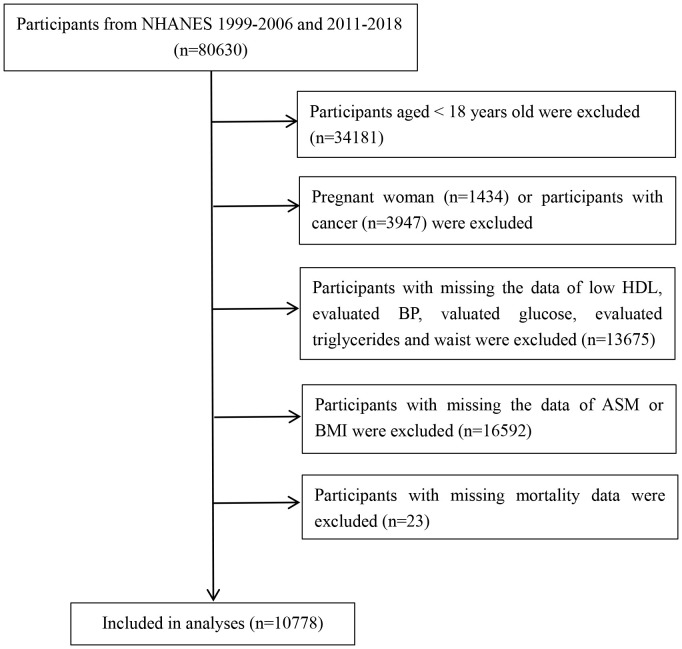
Methods: This study analyzed data from the National Health and Nutrition Examination Survey (NHANES) III for the years 1999-2006 and 2011-2018, and death outcomes were ascertained by linkage to National Death Index (NDI) records through December 31, 2019. Cox proportional hazard models were used to estimate hazard ratios (HRs) and 95% confidence intervals (95% CIs) for all-cause and cardiovascular mortality. In addition, subgroup and sensitivity analyses were conducted to test the robustness of the results.
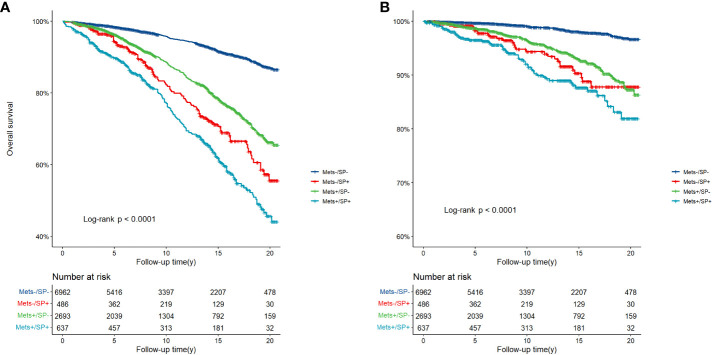
Results: Over a median follow-up period of 13.3 years (95% CI: 12.8-13.8), 1714 deaths were observed. The groups characterized by MetS-/SP+, MetS+/SP-, and MetS+/SP+ exhibited higher all-cause mortality rates in comparison to the MetS-/SP- group, with the MetS+/SP+ group (HR 1.76, 95% CI: 1.37-2.25) displaying the highest all-cause mortality. Increased cardiovascular mortality was observed in the MetS+/SP- (HR 1.84, 95% CI: 1.24-2.72), and MetS+/SP+ groups (HR 2.39, 95% CI: 1.32-4.35) compared to the MetS-/SP- group, whereas it was not statistically significant in the MetS-/SP+ group. However, among males and individuals aged < 60, the presence of both MetS and SP (MetS+/SP+ group) was found to be significantly associated with a higher risk of all-cause and cardiovascular mortality.
Conclusion: The coexistence of MetS and SP increased the risk of all-cause and cardiovascular mortality, particularly in males and in nonelderly populations. Individuals with either MetS or SP may require more careful management to prevent the development of other diseases and thereby reduce mortality.
Keywords: NHANES; all-cause mortality; cardiovascular mortality; metabolic syndrome; sarcopenia.
Copyright © 2024 Huang, Deng, Liu, Ma, Cao, Liu, Wan and Shen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical