

Impact of hospitalized vaso-occlusive crises in the previous calendar year on mortality and complications in adults with sickle cell disease: a French population-based study
- PMID: 38596356
- PMCID: PMC11002849
- DOI: 10.1016/j.lanepe.2024.100901
Impact of hospitalized vaso-occlusive crises in the previous calendar year on mortality and complications in adults with sickle cell disease: a French population-based study
Abstract
Background: Historically, sickle cell disease (SCD) patients experiencing frequent hospitalized vaso-occlusive crises (HVOC) have been associated with increased mortality, yet recent data reflecting the widespread use of hydroxyurea and advancements in disease management remain limited. Our study aims to assess the association between HVOC and mortality or severe complications in patients with SCD in this new treatment landscape.
Methods: This was a retrospective observational cohort study using the French national health data system. Between 01-01-2012 and 12-31-2018, all SCD patients ≥16 years old (ICD-10 codes D57.0-2) were included and followed until 12-31-2018. HVOC was defined as a hospitalization of ≥1 night with primary diagnosis of SCD with crisis, following an emergency room visit. The association between HVOC and severe complications was assessed with a Cox proportional hazards model.
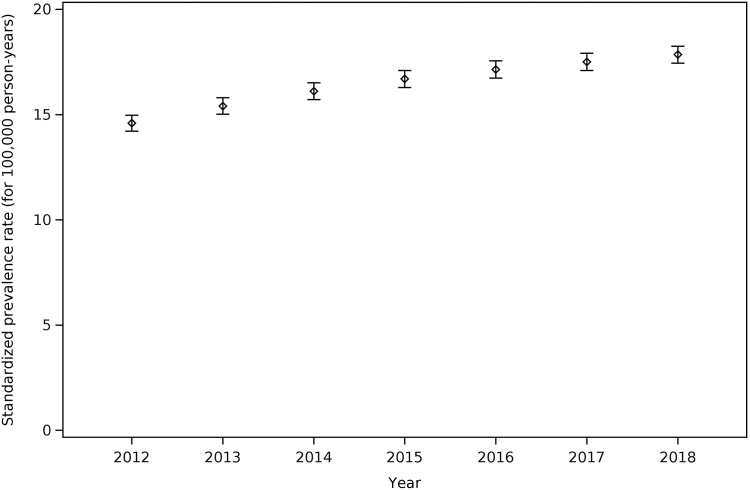
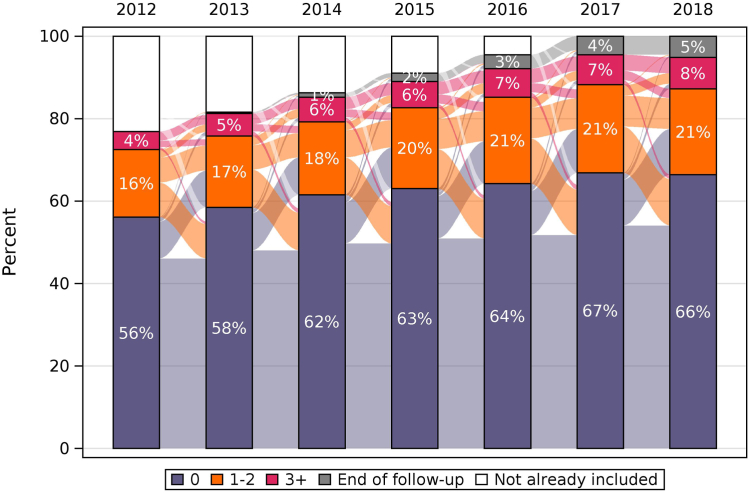
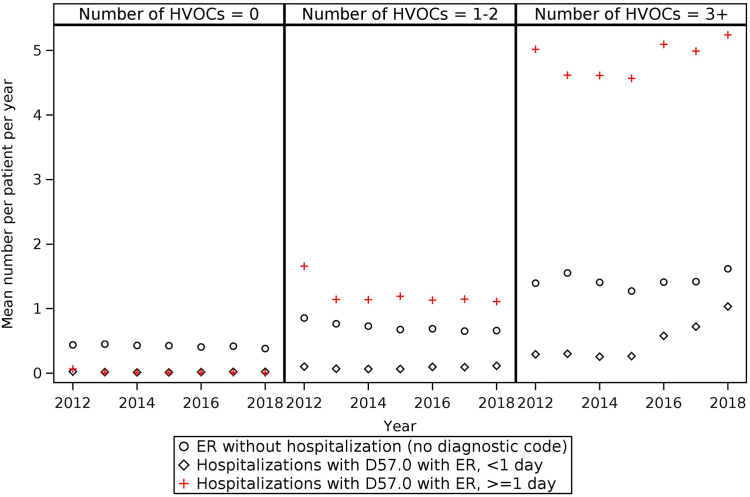
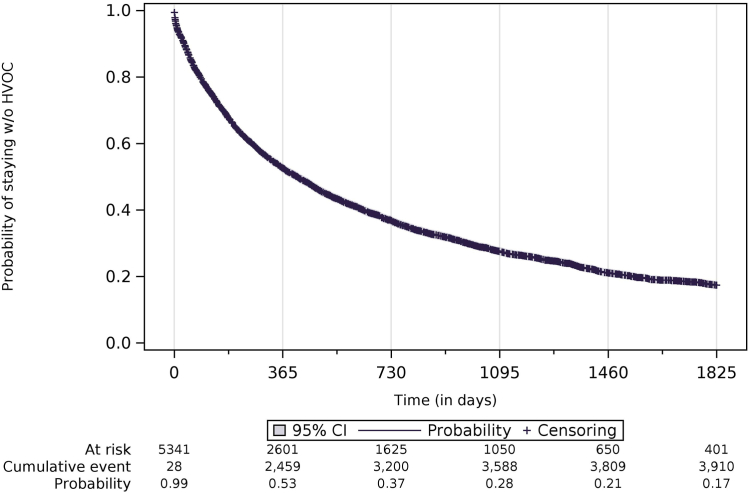
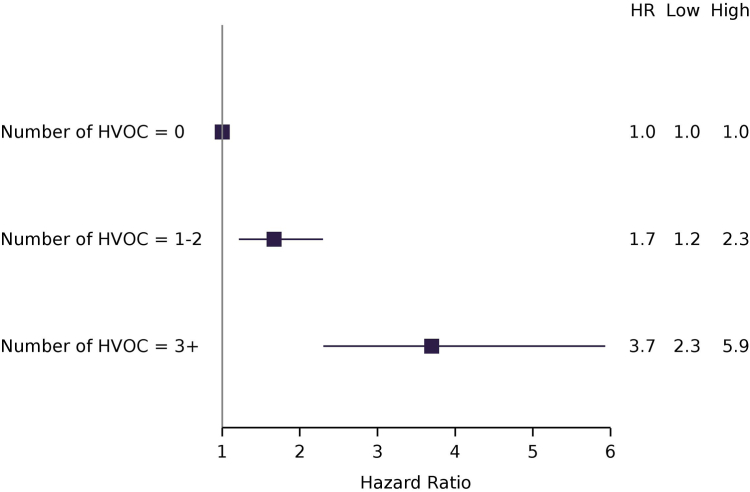
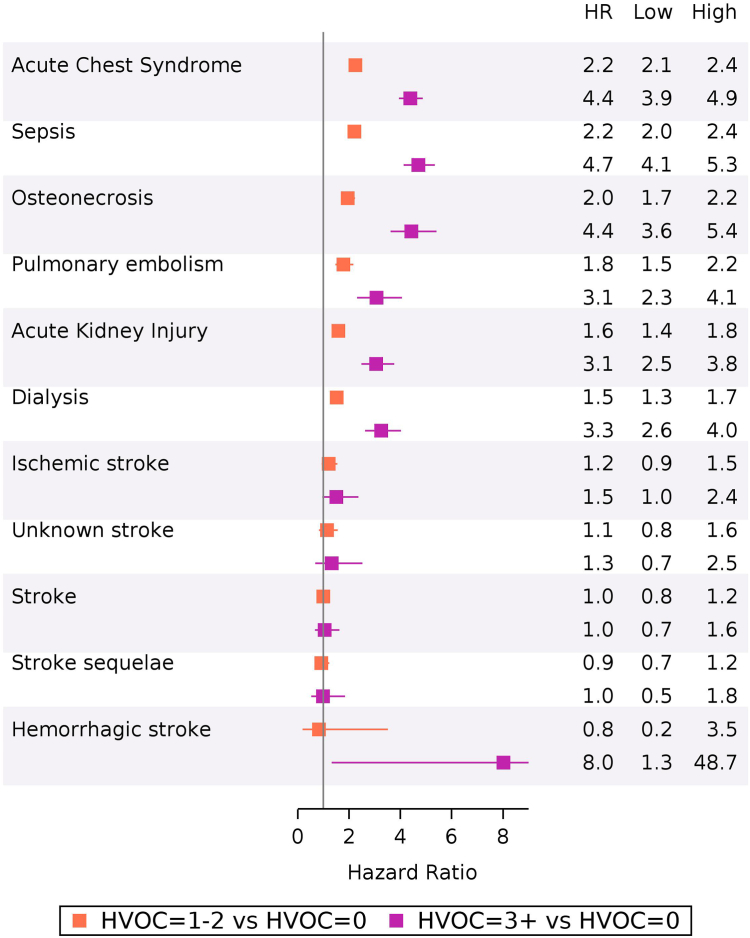
Findings: In total, 8018 patients (56.6% females; 4538/8018) were included. The 2018 SCD standardized one-year period prevalence was 17.9 cases/100,000 person-years [17.4; 18.3]. The mean rate was 0.84 (1.88) HVOC/person-year. In 2018, 70% (5323/7605), 22% (1671/7605), and 8% (611/7605) of patients experienced 0, 1-2, or 3+ HVOCs, respectively. The median survival time between HVOCs was 415 days [386; 439]. Overall, 312 patients died (3.9%) with a mean age of 49.8 (19.4). Compared to patients without HVOC, the hazard ratios of death in patients with 1-2 or 3+ HVOCs the year prior to death were 1.67 [1.21; 2.30] and 3.70 [2.30; 5.93], respectively. Incidence of acute chest syndrome, pulmonary embolism, osteonecrosis, and sepsis increased with the HVOCs category, but not stroke. In 2018, 29.5% (180/611) of patients with 3+ HVOCs did not take hydroxyurea.
Interpretation: Patients must be closely monitored during their hospitalizations to intensify treatment and check treatment compliance. Innovative therapies are also required.
Funding: The study was funded by Novartis.
Keywords: France; Mortality; Sickle cell disease; Vaso-occlusive crisis.
© 2024 The Authors.
Conflict of interest statement
Jean-Benoît Arlet declares that he has received research funding from Theravia, GBT-Pfizer, Novartis, and Vertex, and has been supported at scientific conferences by Novartis France and GBT. Eléonore Herquelot, Fanny Raguideau and Ludovic Lamarsalle work for Heva, the CRO which conducted the study on behalf of Novartis. Pablo Bartolucci declares that he has received research funding and personal fees from Theravia, GBT-Pfizer, Novartis, Vertex and Agios, and he is co-founder of Innovhem.
Figures
References
-
- Bilan d’activité 2021. AFDPHE; 2021. Association Française pour le dépistage et la prévention des handicaps de l’enfant.
-
- Thomson A.M., McHugh T.A., Oron A.P., et al. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000–2021: a systematic analysis from the global burden of disease study 2021. Lancet Haematol. 2023;10(8):e585–e599. doi: 10.1016/S2352-3026(23)00118-7. - DOI - PMC - PubMed
-
- Platt O.S., Thorington B.D., Brambilla D.J., et al. Pain in sickle cell disease. N Engl J Med. 1991;325:11–16. - PubMed
LinkOut - more resources
Full Text Sources
