

Postfracture survival in a population-based study of adults aged ≥66 yr: a call to action at hospital discharge
- PMID: 38596507
- PMCID: PMC11001756
- DOI: 10.1093/jbmrpl/ziae002
Postfracture survival in a population-based study of adults aged ≥66 yr: a call to action at hospital discharge
Abstract
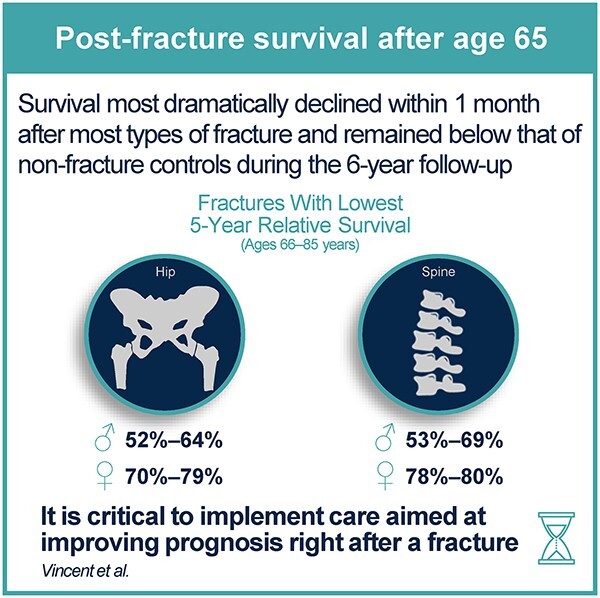
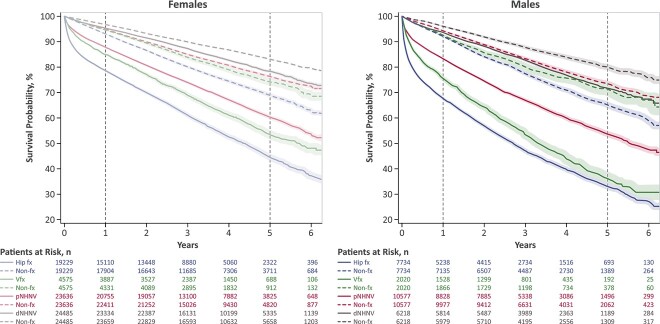
Postfracture survival rates provide prognostic information but are rarely reported along with other mortality outcomes in adults aged ≥50 yr. The timing of survival change following a fracture also needs to be further elucidated. This population-based, matched-cohort, retrospective database study examined 98 474 patients (73% women) aged ≥66 yr with an index fracture occurring at an osteoporotic site (hip, clinical vertebral, proximal non-hip non-vertebral [pNHNV], and distal non-hip non-vertebral [dNHNV]) from 2011 to 2015, who were matched (1:1) to nonfracture individuals based on sex, age, and comorbidities. All-cause 1- and 5-yr overall survival and relative survival ratios (RSRs) were assessed, and time trends in survival changes were characterized starting immediately after a fracture. In both sexes, overall survival was markedly decreased over 6 yr of follow-up after hip, vertebral, and pNHNV fractures, and as expected, worse survival rates were observed in older patients and males. The lowest 5-yr RSRs were observed after hip fractures in males (66-85 yr, 51.9%-63.9%; ≥86 yr, 34.5%), followed by vertebral fractures in males (66-85 yr, 53.2%-69.4%; ≥86 yr, 35.5%), and hip fractures in females (66-85 yr, 69.8%-79.0%; ≥86 yr, 52.8%). Although RSRs did not decrease as markedly after dNHNV fractures in younger patients, relatively low 5-yr RSRs were observed in females (75.9%) and males (69.5%) aged ≥86 yr. The greatest reduction in survival occurred within the initial month after hip, vertebral, and pNHNV fractures, indicating a high relative impact of short-term factors, with survival-reduction effects persisting over time. Therefore, the most critical period for implementing interventions aimed at improving post-fracture prognosis appears to be immediately after a fracture; however, considering the immediate need for introducing such interventions, primary fracture prevention is also crucial to prevent the occurrence of the initial fracture in high-risk patients.
Keywords: aging; fracture prevention; general population studies; osteoporosis; screening.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
E.S. has received consulting fees from Amgen. J.D.A. has received consulting fees from Amgen, Gilead, GlaxoSmithKline, and Paladin; received research funding from Amgen and Radius; and served on speakers bureaus for Amgen, Gilead, and GlaxoSmithKline. J.P.B. has received research support from Mereo BioPharma, Radius Health, and Servier; has served as a consultant for Amgen, Gilead, Paladin, Pfizer, Servier, and Ultragenyx; and has served on speakers bureaus for Amgen. J.-E.T. has led educational workshops for Allergan; received consulting fees from Amgen, Analytica Laser International, AstraZeneca, Bayer, Edwards Lifesciences, the European Commission Initiative on Breast Cancer (ECIBC), Evidera, Flatiron, GSK, Lilly, Merck, Novartis, PCDI Canada, Pfizer Inc., and Roche; and received research funding from Amgen, Assurex/Myriad, AstraZeneca, CSL Behring, Edwards Lifesciences, Novo Nordisk, and Sage. G.V., R.J.W., and N.H. are employees of Amgen and own Amgen stock.
Figures





Similar articles
-
Utilization of DXA Bone Mineral Densitometry in Ontario: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(20):1-180. Epub 2006 Nov 1. Ont Health Technol Assess Ser. 2006. PMID: 23074491 Free PMC article.
-
One-Year Postfracture Mortality Rate in Older Adults With Hip Fractures Relative to Other Lower Extremity Fractures: Retrospective Cohort Study.JMIR Aging. 2022 Mar 16;5(1):e32683. doi: 10.2196/32683. JMIR Aging. 2022. PMID: 35293865 Free PMC article.
-
Rates of osteoporosis screening and treatment following vertebral fracture.Spine J. 2019 Mar;19(3):411-417. doi: 10.1016/j.spinee.2018.08.004. Epub 2018 Aug 22. Spine J. 2019. PMID: 30142455
-
Prediction of clinical non-spine fractures in older black and white men and women with volumetric BMD of the spine and areal BMD of the hip: the Health, Aging, and Body Composition Study*.J Bone Miner Res. 2007 Dec;22(12):1862-8. doi: 10.1359/jbmr.070807. J Bone Miner Res. 2007. PMID: 17708713
-
Epidemiology and predictors of fractures associated with osteoporosis.Am J Med. 1997 Aug 18;103(2A):3S-8S; discussion 8S-11S. doi: 10.1016/s0002-9343(97)90021-8. Am J Med. 1997. PMID: 9302892 Review.
Cited by
-
It is not "just a fracture".JBMR Plus. 2024 Apr 9;8(5):ziae022. doi: 10.1093/jbmrpl/ziae022. eCollection 2024 May. JBMR Plus. 2024. PMID: 38596506 Free PMC article.
-
The efficacy of exercise prescription in patients with osteoporotic fractures: a systematic review and meta-analysis.J Orthop Surg Res. 2025 Mar 7;20(1):250. doi: 10.1186/s13018-025-05636-z. J Orthop Surg Res. 2025. PMID: 40050972 Free PMC article.
-
Association of serum urea-to-creatinine and creatinine-to-cystatin C ratios with bone mineral density and osteoporosis: a cross-sectional study.Sci Rep. 2025 Jul 30;15(1):27774. doi: 10.1038/s41598-025-13037-9. Sci Rep. 2025. PMID: 40739314 Free PMC article.
-
The Fracture Phenotypes in Women and Men of 50 Years and Older with a Recent Clinical Fracture.Curr Osteoporos Rep. 2024 Dec;22(6):611-620. doi: 10.1007/s11914-024-00885-z. Epub 2024 Sep 10. Curr Osteoporos Rep. 2024. PMID: 39254815 Review.
-
High mortality rates after distal femur fractures in patients with end-stage renal disease.OTA Int. 2025 Aug 1;8(3):e421. doi: 10.1097/OI9.0000000000000421. eCollection 2025 Sep. OTA Int. 2025. PMID: 40755548 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
