

Periodontal Treatment During the Blanking Period Improves the Outcome of Atrial Fibrillation Ablation
- PMID: 38597139
- PMCID: PMC11262508
- DOI: 10.1161/JAHA.123.033740
Periodontal Treatment During the Blanking Period Improves the Outcome of Atrial Fibrillation Ablation
Abstract
Background: Periodontitis has not been recognized as a modifiable risk factor for atrial fibrillation (AF). This prospective nonrandomized study investigated whether periodontal treatment improves the AF ablation outcome.
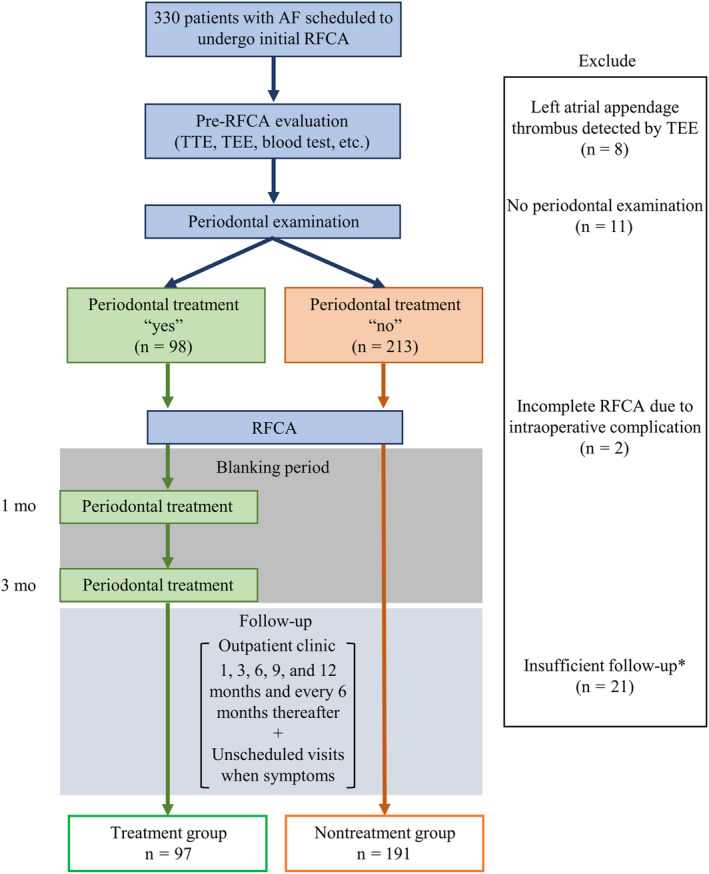
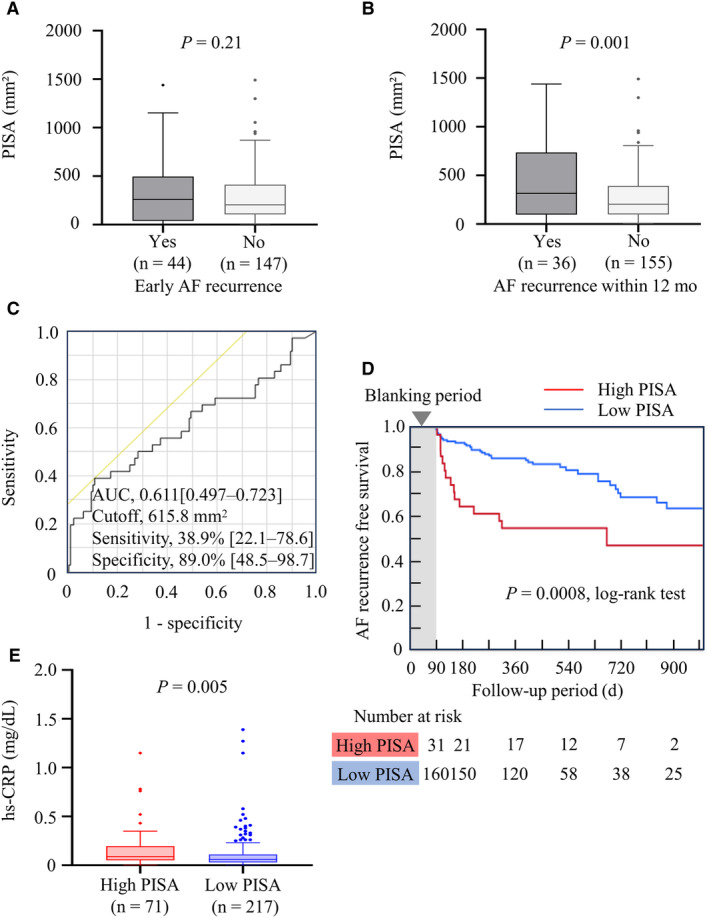
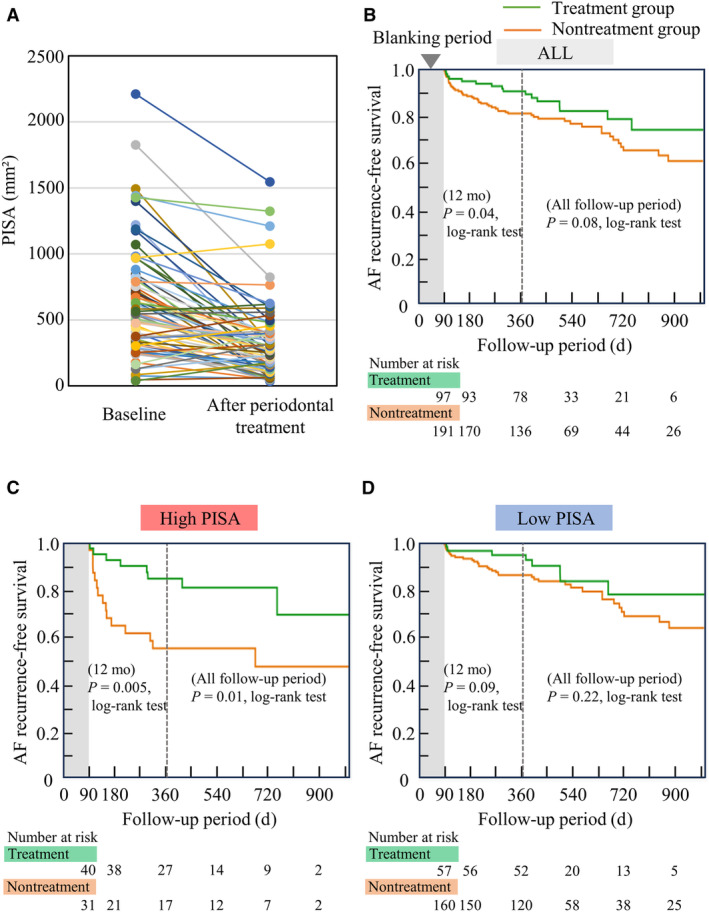
Methods and results: We prospectively enrolled 288 AF patients scheduled to undergo initial radiofrequency catheter ablation. Each patient underwent periodontal inflamed surface area (PISA; a quantitative index of periodontal inflammation) measurement. All eligible patients were recommended to receive periodontal treatment within the blanking period, and 97 consented. During the mean follow-up period of 507±256 days, 70 (24%) AF recurrences were documented. Patients who exhibited AF recurrences had a higher PISA than those who did not (456.8±403.5 versus 277.7±259.0 mm2, P=0.001). These patients were categorized into high-PISA (>615 mm2) and low-PISA (<615 mm2) groups according to the receiver operating characteristic analysis for AF recurrence (area under the curve, 0.611; sensitivity, 39%; specificity, 89%). A high PISA, as well as female sex, AF duration, and left atrial volume, were the statistically significant predicter for AF recurrence (hazard ratio [HR], 2.308 [95% CI, 1.234-4.315]; P=0.009). In patients with a high PISA, those who underwent periodontal treatment showed significantly fewer AF recurrences (P=0.01, log-rank test). The adjusted HR of periodontal treatment for AF recurrence was 0.393 (95% CI, 0.215-0.719; P=0.002).
Conclusions: Periodontitis may serve as a modifiable risk factor for AF. PISA is a hallmark of AF recurrence, and periodontal treatment improves the AF ablation outcome, especially for those with poor periodontal condition.
Keywords: modifiable risk factor; periodontal inflamed surface area; periodontitis; radiofrequency catheter ablation; recurrence.
Figures
Comment in
-
Periodontal treatment reduces AF recurrence.Nat Rev Cardiol. 2024 Jun;21(6):355. doi: 10.1038/s41569-024-01036-8. Nat Rev Cardiol. 2024. PMID: 38664574 No abstract available.
References
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton‐Cheh C, Lubitz SA, Magnani JW, Ellinor PT, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. doi: 10.1016/S0140-6736(14)61774-8 - DOI - PMC - PubMed
-
- Turagam MK, Musikantow D, Whang W, Koruth JS, Miller MA, Langan MN, Sofi A, Choudry S, Dukkipati SR, Reddy VY. Assessment of catheter ablation or antiarrhythmic drugs for first‐line therapy of atrial fibrillation: a meta‐analysis of randomized clinical trials. JAMA Cardiol. 2021;6:697–705. doi: 10.1001/jamacardio.2021.0852 - DOI - PMC - PubMed
-
- Wynn GJ, Das M, Bonnett LJ, Panikker S, Wong T, Gupta D. Efficacy of catheter ablation for persistent atrial fibrillation: a systematic review and meta‐analysis of evidence from randomized and nonrandomized controlled trials. Circ Arrhythm Electrophysiol. 2014;7:841–852. doi: 10.1161/CIRCEP.114.001759 - DOI - PubMed
-
- Chung MK, Eckhardt LL, Chen LY, Ahmed HM, Gopinathannair R, Joglar JA, Noseworthy PA, Pack QR, Sanders P, Trulock KM, et al. Lifestyle and risk factor modification for reduction of atrial fibrillation: a scientific statement from the American Heart Association. Circulation. 2020;141:e750–e772. doi: 10.1161/CIR.0000000000000748 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
