

Short-Term Myopic Defocus and Choroidal Thickness in Children and Adults
- PMID: 38597724
- PMCID: PMC11008753
- DOI: 10.1167/iovs.65.4.22
Short-Term Myopic Defocus and Choroidal Thickness in Children and Adults
Abstract
Purpose: Studies report conflicting findings regarding choroidal thickness changes in response to myopic defocus in humans. This study aimed to investigate the choroidal response to myopic defocus in children and adults using automated analysis.
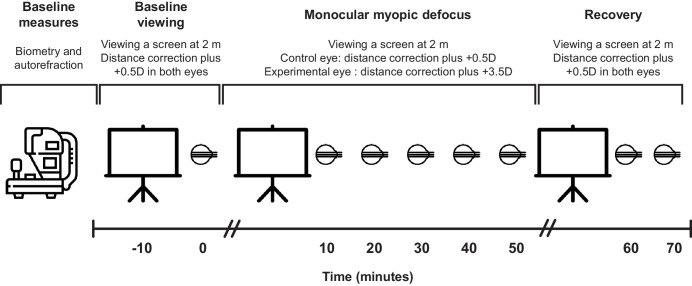
Methods: Participants (N = 46) were distance-corrected in both eyes and viewed a movie on a screen for 10 minutes. Two optical coherence tomography (OCT) radial scans were collected for each eye, then +3 diopters was added to one eye. Participants continued to watch the movie, OCT scans were repeated every 10 minutes for 50 minutes, and then recovery was assessed at 60 and 70 minutes. Defocus was interrupted for approximately two out of each 10 minutes for OCT imaging. OCT images were analyzed using an automated algorithm and trained neural network implemented in MATLAB to determine choroidal thickness at each time point. Repeated-measures ANOVA was used to assess changes with time in three age groups (6-17, 18-30, and 31-45 years) and by refractive error group (myopic and nonmyopic).
Results: Choroidal thickness was significantly associated with spherical equivalent refraction, with the myopic group having a thinner choroid than the nonmyopic group (P < 0.001). With imposed myopic defocus, there were no significant changes in choroidal thickness at any time point for any age group and for either refractive error group (P > 0.05 for all).
Conclusions: Findings demonstrate that, using the described protocol, the choroidal thickness of children and adults does not significantly change in response to short-term, full-field myopic defocus, in contrast to several previously published studies.
Conflict of interest statement
Disclosure:
Figures




References
-
- Holden BA, Fricke TR, Wilson DA, et al. .. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016; 123: 1036–1042. - PubMed
-
- Saw SM, Gazzard G, Shih-Yen EC, Chua WH.. Myopia and associated pathological complications. Ophthalmic Physiol Opt. 2005; 25: 381–391. - PubMed
-
- Grodum K, Heijl A, Bengtsson B.. Refractive error and glaucoma. Acta Ophthalmol Scand. 2001; 79: 560–566. - PubMed
-
- Lim R, Mitchell P, Cumming RG.. Refractive associations with cataract: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 1999; 40: 3021–3026. - PubMed
-
- Polkinghorne PJ, Craig JP.. Northern New Zealand Rhegmatogenous Retinal Detachment Study: epidemiology and risk factors. Clin Exp Ophthalmol. 2004; 32: 159–163. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
