

Clinical and neuroanatomical characterization of the semantic behavioral variant of frontotemporal dementia in a multicenter Italian cohort
- PMID: 38597943
- PMCID: PMC11233398
- DOI: 10.1007/s00415-024-12338-9
Clinical and neuroanatomical characterization of the semantic behavioral variant of frontotemporal dementia in a multicenter Italian cohort
Abstract
Background: Semantic behavioral variant frontotemporal dementia (sbvFTD) is a neurodegenerative condition presenting with specific behavioral and semantic derangements and predominant atrophy of the right anterior temporal lobe (ATL). The objective was to evaluate clinical, neuropsychological, neuroimaging, and genetic features of an Italian sbvFTD cohort, defined according to recently proposed guidelines, compared to semantic variant primary progressive aphasia (svPPA) and behavioral variant FTD (bvFTD) patients.
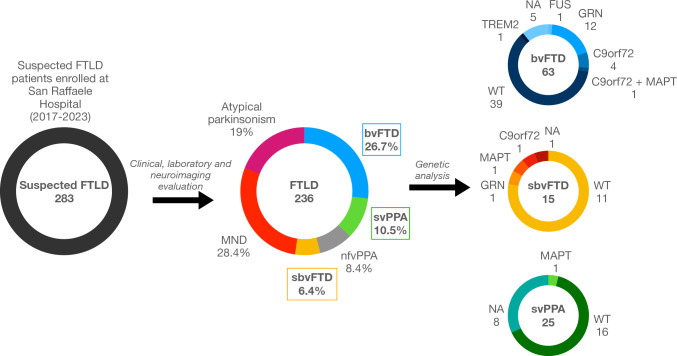
Methods: Fifteen sbvFTD, sixty-three bvFTD, and twenty-five svPPA patients and forty controls were enrolled. Patients underwent clinical, cognitive evaluations, and brain MRI. Symptoms of bvFTD patients between onset and first visit were retrospectively recorded and classified as early and late. Grey matter atrophy was investigated using voxel-based morphometry.
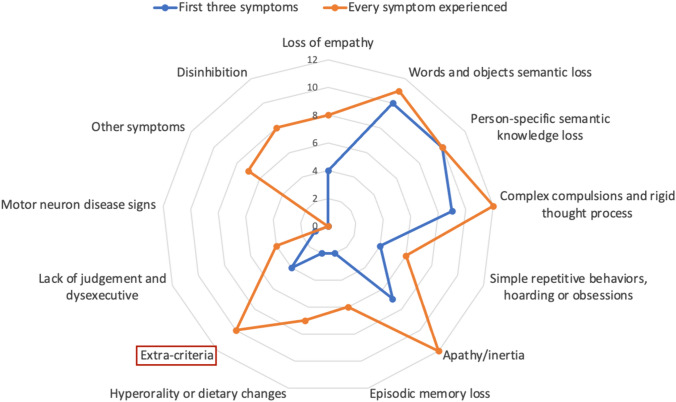
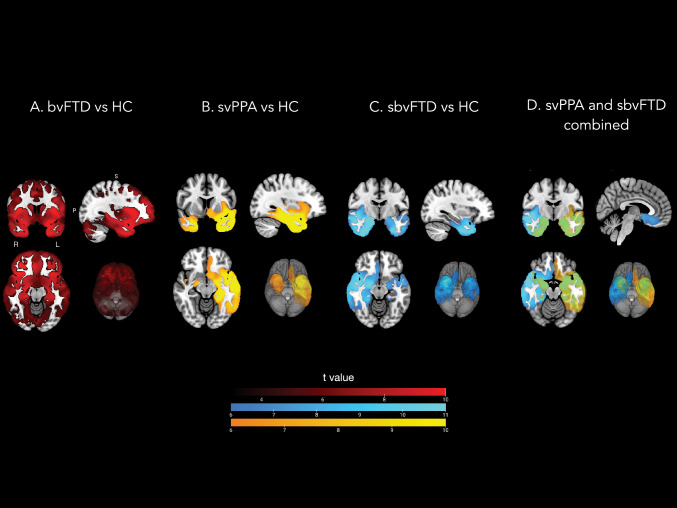
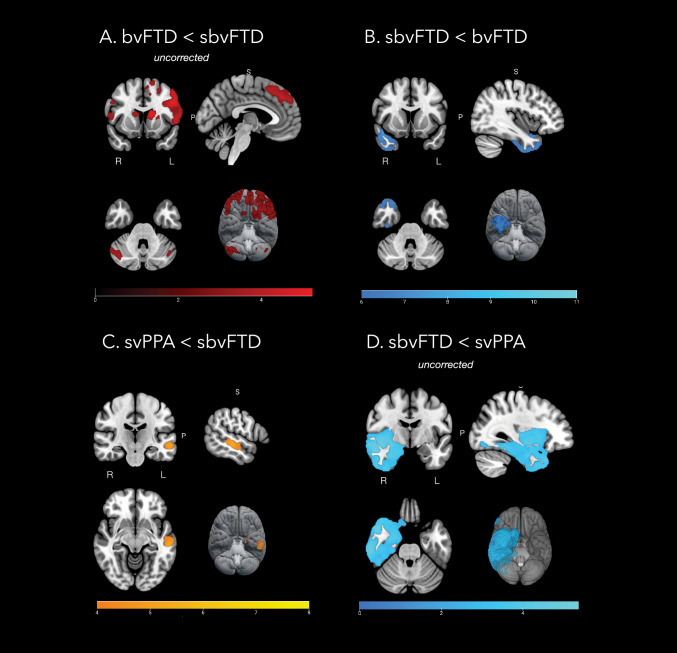
Results: sbvFTD experienced early criteria-specific symptoms: world, object and person-specific semantic loss (67%), complex compulsions and rigid thought (60%). Sequentially, more behavioral symptoms emerged (apathy/inertia, loss of empathy) along with non-criteria-specific symptoms (anxiety, suspiciousness). sbvFTD showed sparing of attentive/executive functions, especially compared to bvFTD and better language functions compared to svPPA. All sbvFTD patients failed at the famous face recognition test and more than 80% failed in understanding written metaphors and humor. At MRI, sbvFTD had predominant right ATL atrophy, almost specular to svPPA. Three sbvFTD patients presented pathogenic genetic variants.
Conclusion: We replicated the application of sbvFTD diagnostic guidelines in an independent Italian cohort, demonstrating that the presence of person-specific semantic knowledge loss and mental rigidity, along with preserved executive functions and a predominant right ATL atrophy with sparing of frontal lobes, should prompt a diagnosis of sbvFTD.
Keywords: FTD; MRI; Voxel-based morphometry; rtvFTD; sbvFTD.
© 2024. The Author(s).
Conflict of interest statement
A. Ghirelli and E.G. Spinelli has nothing to disclose. E. Canu has received research supports from the Italian Ministry of Health. S. Basaia has received research supports from the Italian Ministry of Health. V. Castelnovo, G. Cecchetti, E. Sibilla, T. Domi, G. Magnani, F. Caso, P. Caroppo, S. Prioni, C. Villa, G. Rossi, L. Tremolizzo, I. Apollonio, F. Verde, N. Ticozzi, and V. Silani has nothing to disclose. M. Filippi is Editor-in-Chief of the Journal of Neurology; Associate Editor of Human Brain Mapping, Neurological Sciences, and Radiology; received compensation for consulting services from Alexion, Almirall, Biogen, Merck, Novartis, Roche, Sanofi, speaking activities from Bayer, Biogen, Celgene, Chiesi Italia SpA, Eli Lilly, Genzyme, Janssen, Merck-Serono, Neopharmed Gentili, Novartis, Novo Nordisk, Roche, Sanofi, Takeda, and TEVA, participation in Advisory Boards for Alexion, Biogen, Bristol-Myers Squibb, Merck, Novartis, Roche, Sanofi, Sanofi-Aventis, Sanofi-Genzyme, Takeda, scientific direction of educational events for Biogen, Merck, Roche, Celgene, Bristol-Myers Squibb, Lilly, Novartis, Sanofi-Genzyme; he receives research support from Biogen Idec, Merck-Serono, Novartis, Roche, the Italian Ministry of Health, the Italian Ministry of University and Research, and Fondazione Italiana Sclerosi Multipla. F. Agosta is Associate Editor of NeuroImage: Clinical; has received speaker honoraria from Biogen Idec, Italfarmaco, Roche, Zambon and Eli Lilly; and receives or has received research supports from the Italian Ministry of Health, the Italian Ministry of University and Research, AriSLA (Fondazione Italiana di Ricerca per la SLA), the European Research Council, the EU Joint Programme—Neurodegenerative Disease Research (JPND), and Foundation Research on Alzheimer Disease (France).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
