

Effects of restrictive fluid therapy on the time to resolution of hyperlactatemia in ICU patients with septic shock. A secondary post hoc analysis of the CLASSIC randomized trial
- PMID: 38598125
- PMCID: PMC11078841
- DOI: 10.1007/s00134-024-07385-9
Effects of restrictive fluid therapy on the time to resolution of hyperlactatemia in ICU patients with septic shock. A secondary post hoc analysis of the CLASSIC randomized trial
Abstract
Purpose: The aim of this study was to examine the effects of intravenous (IV) fluid restriction on time to resolution of hyperlactatemia in septic shock. Hyperlactatemia in sepsis is associated with worse outcome. Sepsis guidelines suggest targeting lactate clearance to guide fluid therapy despite the complexity of hyperlactatemia and the potential harm of fluid overload.
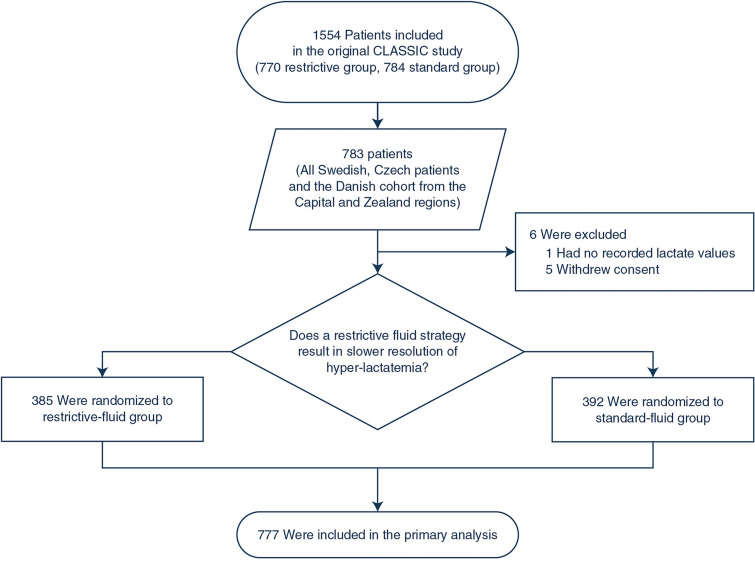
Methods: We conducted a post hoc analysis of serial plasma lactate concentrations in a sub-cohort of 777 patients from the international multicenter clinical CLASSIC trial (restriction of intravenous fluids in intensive care unit (ICU) patients with septic shock). Adult ICU patients with septic shock had been randomized to restrictive (n = 385) or standard (n = 392) intravenous fluid therapy. The primary outcome, time to resolution of hyperlactatemia, was analyzed with a competing-risks regression model. Death and discharge were competing outcomes, and administrative censoring was imposed 72 h after randomization if hyperlactatemia persisted. The regression analysis was adjusted for the same stratification variables and covariates as in the original CLASSIC trial analysis.
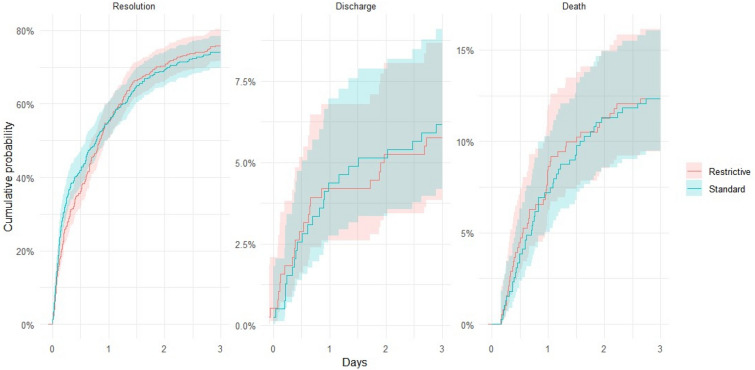
Results: The hazard ratios (HRs) for the cumulative probability of resolution of hyperlactatemia, in the restrictive vs the standard group, in the unadjusted analysis, with time split, were 0.94 (confidence interval (CI) 0.78-1.14) at day 1 and 1.21 (0.89-1.65) at day 2-3. The adjusted analyses were consistent with the unadjusted results.
Conclusion: In this post hoc retrospective analysis of a multicenter randomized controlled trial (RCT), a restrictive intravenous fluid strategy did not seem to affect the time to resolution of hyperlactatemia in adult ICU patients with septic shock.
Keywords: Fluid therapy; Hyperlactatemia; Lactate; Sepsis; Septic shock.
© 2024. The Author(s).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):775–787. doi: 10.1001/jama.2016.0289. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
