

Atrial Fibrillation and Clonal Hematopoiesis in TET2 and ASXL1
- PMID: 38598228
- PMCID: PMC11007653
- DOI: 10.1001/jamacardio.2024.0459
Atrial Fibrillation and Clonal Hematopoiesis in TET2 and ASXL1
Abstract
Importance: Clonal hematopoiesis of indeterminate potential (CHIP) may contribute to the risk of atrial fibrillation (AF) through its association with inflammation and cardiac remodeling.
Objective: To determine whether CHIP was associated with AF, inflammatory and cardiac biomarkers, and cardiac structural changes.
Design, setting, and participants: This was a population-based, prospective cohort study in participants of the Atherosclerosis Risk in Communities (ARIC) study and UK Biobank (UKB) cohort. Samples were collected and echocardiography was performed from 2011 to 2013 in the ARIC cohort, and samples were collected from 2006 to 2010 in the UKB cohort. Included in this study were adults without hematologic malignancies, mitral valve stenosis, or previous mitral valve procedure from both the ARIC and UKB cohorts; additionally, participants without hypertrophic cardiomyopathy and congenital heart disease from the UKB cohort were also included. Data analysis was completed in 2023.
Exposures: CHIP (variant allele frequency [VAF] ≥2%), common gene-specific CHIP subtypes (DNMT3A, TET2, ASXL1), large CHIP (VAF ≥10%), inflammatory and cardiac biomarkers (high-sensitivity C-reactive protein, interleukin 6 [IL-6], IL-18, high-sensitivity troponin T [hs-TnT] and hs-TnI, N-terminal pro-B-type natriuretic peptide), and echocardiographic indices.
Main outcome measure: Incident AF.
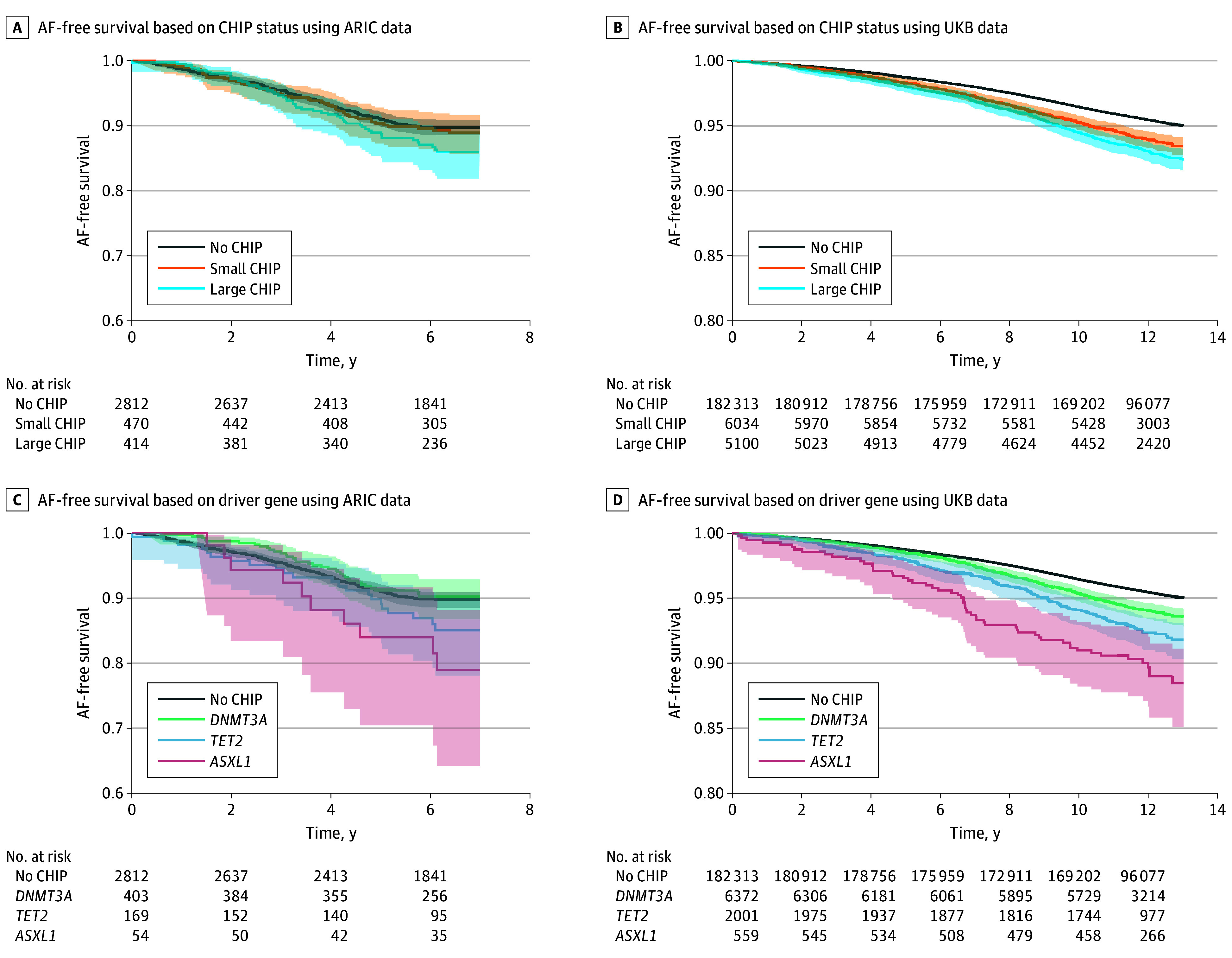
Results: A total of 199 982 adults were included in this study. In ARIC participants (4131 [2.1%]; mean [SD] age, 76 [5] years; 2449 female [59%]; 1682 male [41%]; 935 Black [23%] and 3196 White [77%]), 1019 had any CHIP (24.7%), and 478 had large CHIP (11.6%). In UKB participants (195 851 [97.9%]; mean [SD] age, 56 [8] years; 108 370 female [55%]; 87 481 male [45%]; 3154 Black [2%], 183 747 White [94%], and 7971 other race [4%]), 11 328 had any CHIP (5.8%), and 5189 had large CHIP (2.6%). ARIC participants were followed up for a median (IQR) period of 7.0 (5.3-7.7) years, and UKB participants were followed up for a median (IQR) period of 12.2 (11.3-13.0) years. Meta-analyzed hazard ratios for AF were 1.12 (95% CI, 1.01-1.25; P = .04) for participants with vs without large CHIP, 1.29 (95% CI, 1.05-1.59; P = .02) for those with vs without large TET2 CHIP (seen in 1340 of 197 209 [0.67%]), and 1.45 (95% CI, 1.02-2.07; P = .04) for those with vs without large ASXL1 CHIP (seen in 314 of 197 209 [0.16%]). Large TET2 CHIP was associated with higher IL-6 levels. Additionally, large ASXL1 was associated with higher hs-TnT level and increased left ventricular mass index.
Conclusions and relevance: Large TET2 and ASXL1, but not DNMT3A, CHIP was associated with higher IL-6 level, indices of cardiac remodeling, and increased risk for AF. Future research is needed to elaborate on the mechanisms driving the associations and to investigate potential interventions to reduce the risk.
Conflict of interest statement
Figures



References
-
- Roth GA, Mensah GA, Johnson CO, et al. ; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group . Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982-3021. doi:10.1016/j.jacc.2020.11.010 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
