

Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies
- PMID: 38599681
- PMCID: PMC11103301
- DOI: 10.1136/bjsports-2023-107849
Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies
Abstract
Objective: To examine and summarise evidence from meta-analyses of cohort studies that evaluated the predictive associations between baseline cardiorespiratory fitness (CRF) and health outcomes among adults.
Design: Overview of systematic reviews.
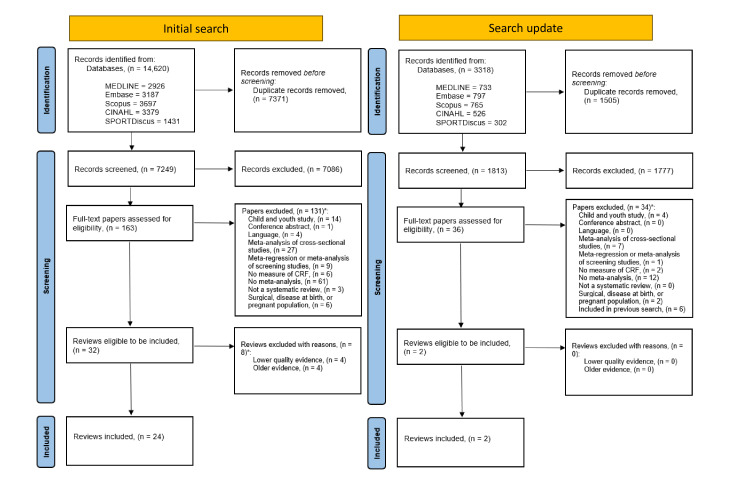
Data source: Five bibliographic databases were searched from January 2002 to March 2024.
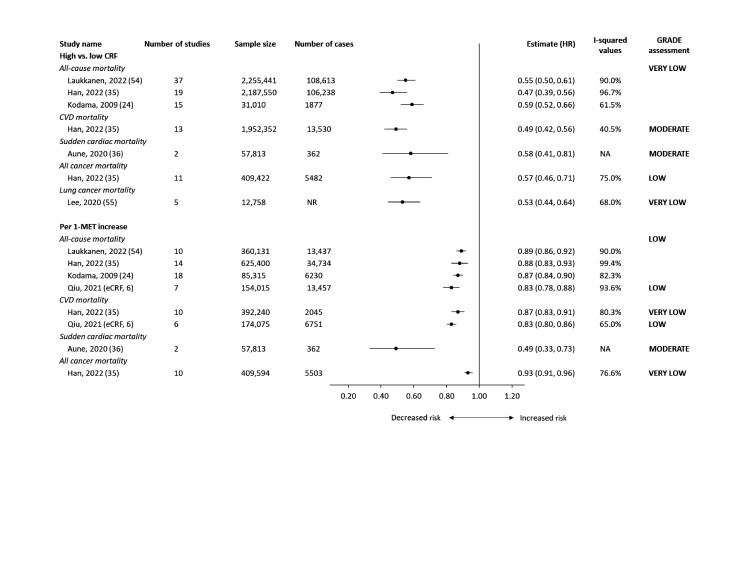
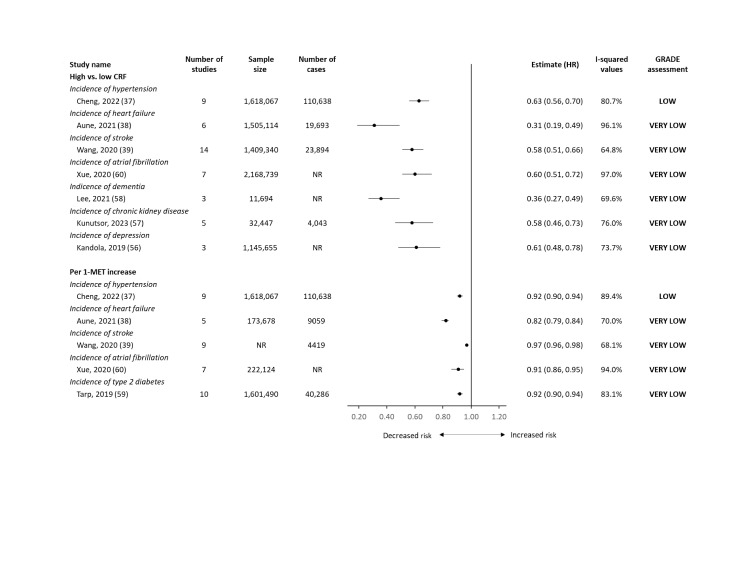
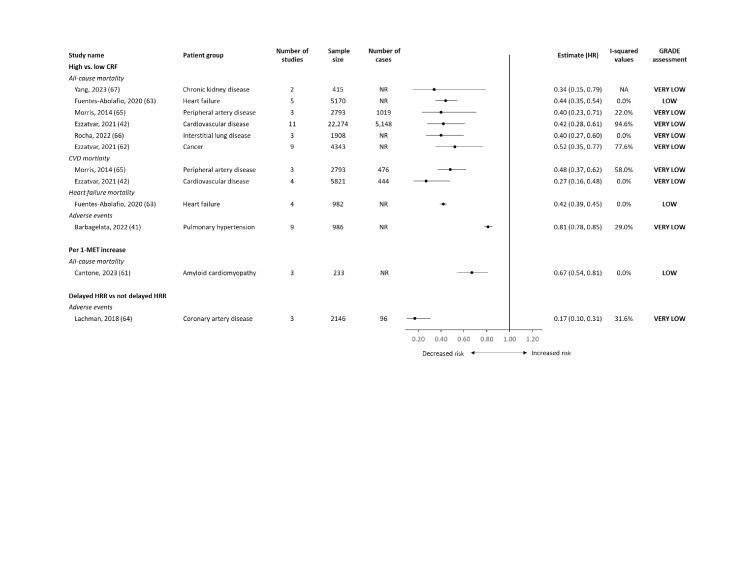
Results: From the 9062 papers identified, we included 26 systematic reviews. We found eight meta-analyses that described five unique mortality outcomes among general populations. CRF had the largest risk reduction for all-cause mortality when comparing high versus low CRF (HR=0.47; 95% CI 0.39 to 0.56). A dose-response relationship for every 1-metabolic equivalent of task (MET) higher level of CRF was associated with a 11%-17% reduction in all-cause mortality (HR=0.89; 95% CI 0.86 to 0.92, and HR=0.83; 95% CI 0.78 to 0.88). For incident outcomes, nine meta-analyses described 12 unique outcomes. CRF was associated with the largest risk reduction in incident heart failure when comparing high versus low CRF (HR=0.31; 95% CI 0.19 to 0.49). A dose-response relationship for every 1-MET higher level of CRF was associated with a 18% reduction in heart failure (HR=0.82; 95% CI 0.79 to 0.84). Among those living with chronic conditions, nine meta-analyses described four unique outcomes in nine patient groups. CRF was associated with the largest risk reduction for cardiovascular mortality among those living with cardiovascular disease when comparing high versus low CRF (HR=0.27; 95% CI 0.16 to 0.48). The certainty of the evidence across all studies ranged from very low-to-moderate according to Grading of Recommendations, Assessment, Development and Evaluations.
Conclusion: We found consistent evidence that high CRF is strongly associated with lower risk for a variety of mortality and incident chronic conditions in general and clinical populations.
Keywords: Cardiovascular Diseases; Cohort Studies; Physical fitness; Review.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Balady GJ, Arena R, Sietsema K, et al. American heart Association exercise, cardiac rehabilitation and prevention committee of the Council on clinical cardiology; Council on epidemiology and prevention; Council on peripheral vascular disease; Interdisciplinary Council on quality of care and outcomes research. clinician’s guide to cardiopulmonary exercise testing in adults: a scientific statement from the American heart Association. Circulation 2010;22:191–225. 10.1161/CIR.0b013e3181e52e69 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous