

Age-stratified comorbid and pharmacologic analysis of patients with glioblastoma
- PMID: 38600951
- PMCID: PMC11004500
- DOI: 10.1016/j.bbih.2024.100753
Age-stratified comorbid and pharmacologic analysis of patients with glioblastoma
Abstract
Background: Increased age is a strong and unfavorable prognostic factor for patients with glioblastoma (GBM). However, the relationships between stratified patient age, comorbidities, and medications have yet to be explored in GBM patient survival analyses.
Objective: To evaluate co-morbid conditions, tumor-related symptoms, medication prescriptions, and subject age for patients with GBM and to establish potential targets for prospective studies.
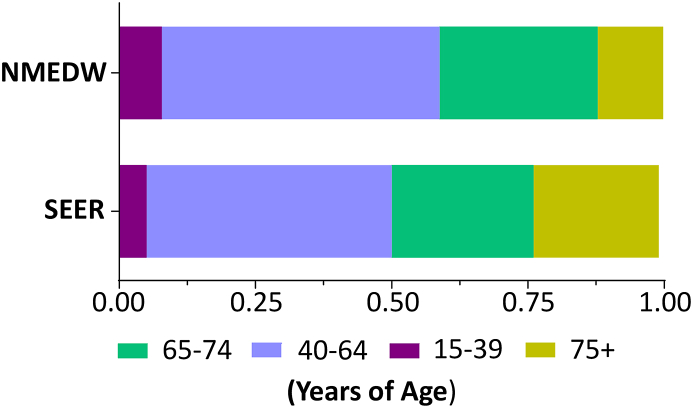
Methods: Electronic health records for 565 patients with IDHwt GBM were evaluated at a single center between January 1, 2000 and August 9, 2021 were retrospectively assessed. Data were stratified by MGMT promoter methylation status when available and were used to construct multivariable time-dependent cox models and intra-cohort hazards.
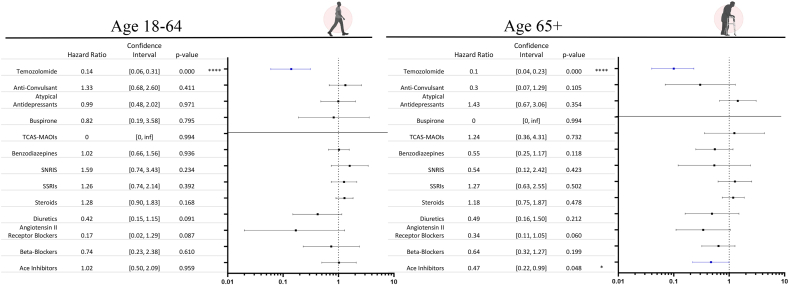
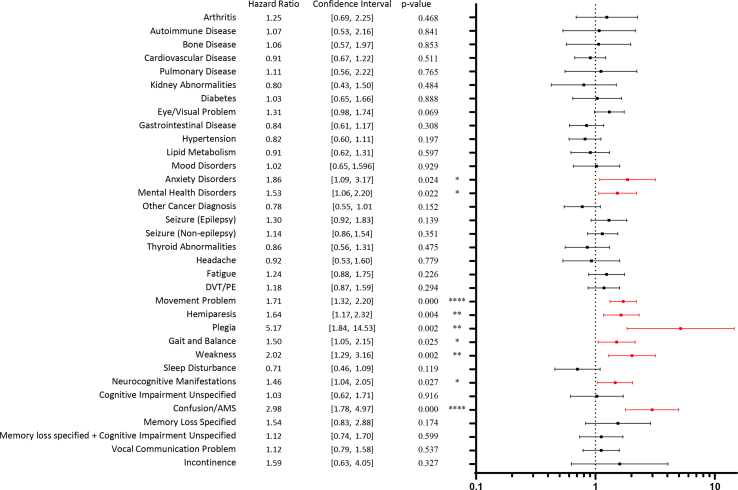
Results: Younger (<65 years of age) but not older (≥65 years) GBM patients demonstrated a worse prognosis with movement related disabilities (P < 0.0001), gait/balance difficulty (P = 0.04) and weakness (P = 0.007), as well as psychiatric conditions, mental health disorders (P = 0.002) and anxiety (P = 0.001). In contrast, older but not younger GBM patients demonstrated a worse prognosis with epilepsy (P = 0.039). Both groups had worse survival with confusion/altered mental status (P = 0.023 vs < 0.000) and an improved survival with a Temozolomide prescription. Older but not younger GBM patients experienced an improved hazard with a prescription of ace-inhibitor medications (P = 0.048).
Conclusion: Age-dependent novel associations between clinical symptoms and medications prescribed for co-morbid conditions were demonstrated in patients with GBM. The results of the current work support future mechanistic studies that investigate the negative relationship(s) between increased age, comorbidities, and drug therapies for differential clinical decision-making across the lifespan of patients with GBM.
Keywords: Confusion; Delirium; Dementia; Elderly; Glioma.
© 2024 Published by Elsevier Inc.
Conflict of interest statement
All co-authors report no financial or otherwise conflicts of interest.
Figures






References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
