

Impact of preterm birth on kidney health and development
- PMID: 38601116
- PMCID: PMC11004308
- DOI: 10.3389/fmed.2024.1363097
Impact of preterm birth on kidney health and development
Abstract
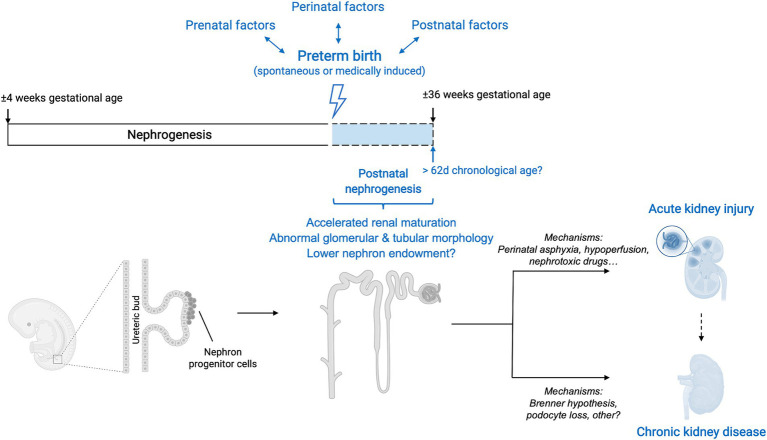
Preterm birth, defined as birth before the gestational age of 37 weeks, affects 11% of the newborns worldwide. While extensive research has focused on the immediate complications associated with prematurity, emerging evidence suggests a link between prematurity and the development of kidney disease later in life. It has been demonstrated that the normal course of kidney development is interrupted in infants born prematurely, causing an overall decrease in functional nephrons. Yet, the pathogenesis leading to the alterations in kidney development and the subsequent pathophysiological consequences causing kidney disease on the long-term are incompletely understood. In the present review, we discuss the current knowledge on nephrogenesis and how this process is affected in prematurity. We further discuss the epidemiological evidence and experimental data demonstrating the increased risk of kidney disease in these individuals and highlight important knowledge gaps. Importantly, understanding the intricate interplay between prematurity, abnormal kidney development, and the long-term risk of kidney disease is crucial for implementing effective preventive and therapeutic strategies.
Keywords: acute kidney injury; chronic kidney disease; nephrogenesis; nephron; premature infant; preterm birth.
Copyright © 2024 Deffrennes, Rayyan, Fidlers, van den Heuvel, Levtchenko and Arcolino.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The impact of intrauterine growth restriction and prematurity on nephron endowment.Nat Rev Nephrol. 2023 Apr;19(4):218-228. doi: 10.1038/s41581-022-00668-8. Epub 2023 Jan 16. Nat Rev Nephrol. 2023. PMID: 36646887 Review.
-
Short-term gestation, long-term risk: prematurity and chronic kidney disease.Pediatrics. 2013 Jun;131(6):1168-79. doi: 10.1542/peds.2013-0009. Epub 2013 May 13. Pediatrics. 2013. PMID: 23669525 Review.
-
Preterm birth and the kidney: implications for long-term renal health.Reprod Sci. 2011 Apr;18(4):322-33. doi: 10.1177/1933719111401659. Reprod Sci. 2011. PMID: 21427457 Review.
-
The long-term renal and cardiovascular consequences of prematurity.Nat Rev Nephrol. 2012 Feb 28;8(5):265-74. doi: 10.1038/nrneph.2012.38. Nat Rev Nephrol. 2012. PMID: 22371245 Review.
-
Kidney growth following preterm birth: evaluation with renal parenchyma ultrasonography.Pediatr Res. 2023 Apr;93(5):1302-1306. doi: 10.1038/s41390-022-01970-8. Epub 2022 Feb 4. Pediatr Res. 2023. PMID: 35121851 Free PMC article.
Cited by
-
Role of rh-IGF-1/IGFBP-3 in the postnatal kidney maturation of preterm pigs: Not so simple.Pediatr Res. 2024 Dec;96(7):1543-1544. doi: 10.1038/s41390-024-03426-7. Epub 2024 Aug 12. Pediatr Res. 2024. PMID: 39134761 Free PMC article. No abstract available.
-
Radial Expansion of the Nephrogenic Zone in the Fetal Human Kidney During Advanced Pregnancy: A Microanatomical Look at a Little Noticed Process.Int J Nephrol. 2025 Mar 20;2025:7571982. doi: 10.1155/ijne/7571982. eCollection 2025. Int J Nephrol. 2025. PMID: 40151636 Free PMC article.
-
Case-control study on long-term kidney outcomes in very low birth weight infants: impact of growth restriction and maternal preeclampsia.J Pediatr (Rio J). 2025 May-Jun;101(3):400-406. doi: 10.1016/j.jped.2025.01.002. Epub 2025 Feb 28. J Pediatr (Rio J). 2025. PMID: 39875102 Free PMC article.
-
Preterm Birth and Kidney Health: From the Womb to the Rest of Life.Children (Basel). 2024 Oct 2;11(10):1213. doi: 10.3390/children11101213. Children (Basel). 2024. PMID: 39457178 Free PMC article. Review.
-
Current status and future directions of application of urine proteomics in neonatology.Front Pediatr. 2025 Jan 14;12:1509468. doi: 10.3389/fped.2024.1509468. eCollection 2024. Front Pediatr. 2025. PMID: 39877338 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources