

A simple and safe surgical technique for nonpalpable lung tumors: One-stop Solution for a nonpalpable lung tumor, Marking, Resection, and Confirmation of the surgical margin in a Hybrid operating room (OS-MRCH)
- PMID: 38601444
- PMCID: PMC11002500
- DOI: 10.21037/tlcr-24-25
A simple and safe surgical technique for nonpalpable lung tumors: One-stop Solution for a nonpalpable lung tumor, Marking, Resection, and Confirmation of the surgical margin in a Hybrid operating room (OS-MRCH)
Abstract
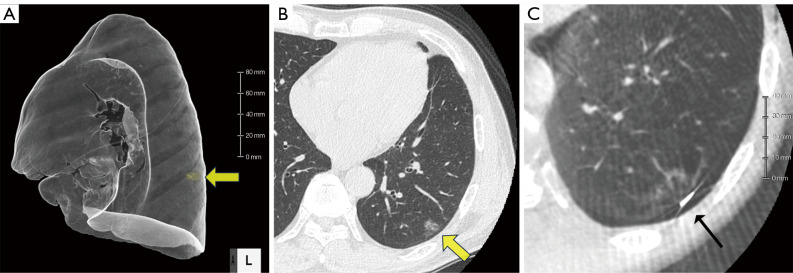
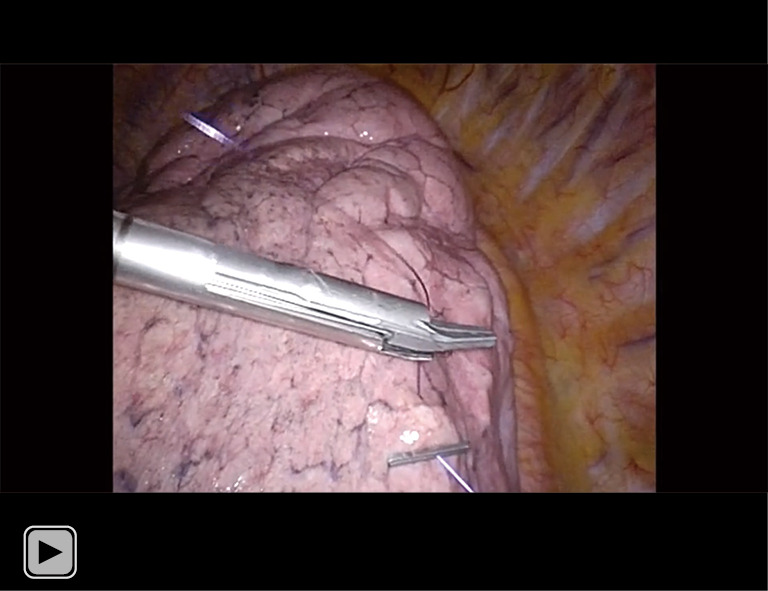
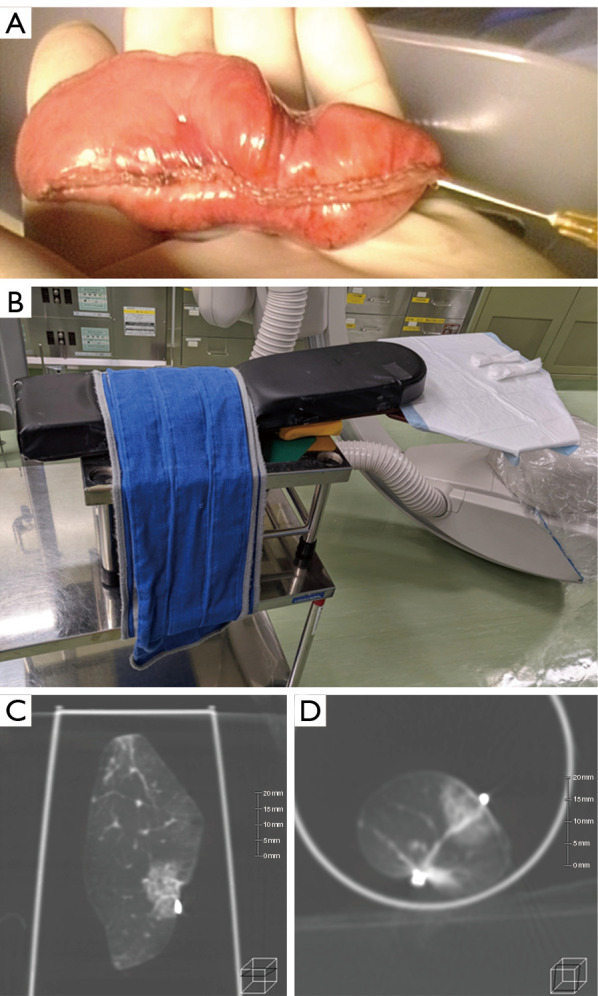
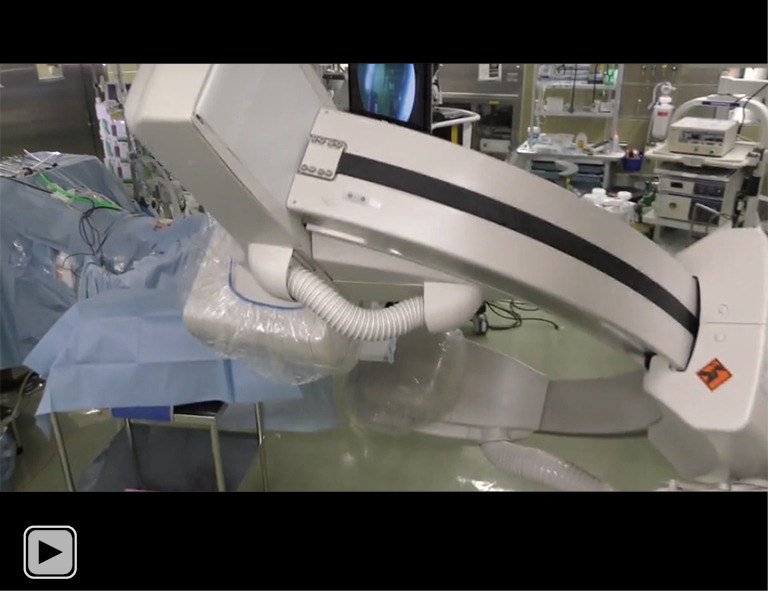
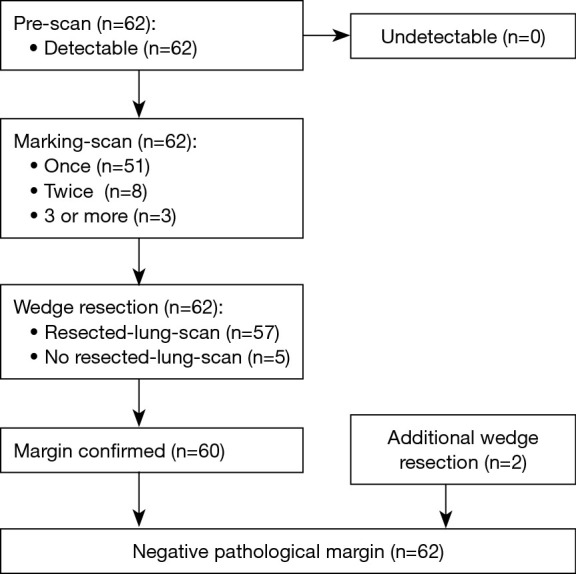
When performing thoracoscopic partial resections of nonpalpable lung tumors such as ground-glass opacities (GGOs) and small tumors, detecting the location of the lesion and assessing the resection margins can be challenging. We have developed a novel method to ease this difficulty, the One-stop Solution for a nonpalpable lung tumor, Marking, Resection, and Confirmation of the surgical margin in a Hybrid operating room (OS-MRCH), which uses a hybrid operating room wherein the operating table is seamlessly integrated with cone-beam computed tomography (CBCT). We performed the OS-MRCH method on 62 nodules including primary lung cancer presenting with GGO. Identification of the lesion and confirmation of the margin were performed in 58 of the cases, while nodules were detected in all. The frequency of computed tomography (CT) scans performed prior to resection was one time in 51 cases, two times in eight cases, and ≥3 times in three cases. Additional resection was performed in two cases. The median operative time was 85.0 minutes, and the median pathological margin was 11.0 mm. The key advantages of this method are that all surgical processes can be completed in a single session, specialized skill sets are not required, and it is feasible to perform in any facility equipped with a hybrid operating room. To overcome its disadvantages, such as longer operating time and limited patient positioning, we devised various methods for positioning patients and for CT imaging of the resected specimens. OS-MRCH is a simple, useful, and practical method for performing thoracoscopic partial resection of nonpalpable lung tumors.
Keywords: Nonpalpable lung tumor; ground-glass opacity (GGO); hybrid operating room; surgical margin; video-assisted thoracoscopic surgery (VATS).
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-25/coif). The authors have no conflicts of interest to declare.
Figures

References
-
- Oikawa T, Nomoto Y, Kinoshita K. A case of left-sided hemiplegia due to cerebral air embolism caused by CT-guided marking for small peripheral lung cancer. The Journal of the Japanese Association for Chest Surgery 2008;22:914-9.
LinkOut - more resources
Full Text Sources