

MRl and MRS hints for the differentiation of cerebellar multiple system atrophy from spinocerebellar ataxia type II
- PMID: 38601670
- PMCID: PMC11004415
- DOI: 10.1016/j.heliyon.2024.e29265
MRl and MRS hints for the differentiation of cerebellar multiple system atrophy from spinocerebellar ataxia type II
Abstract
Background and objectives: The differentiation of spinocerebellar ataxia type II (SCA 2) from idiopathic multiple systemic atrophy of the cerebellar type (MSA-C) is often difficult in patients with cerebellar ataxia when molecular testing is not available. Besides genetic testing, magnetic resonance imagining (MRI) and magnetic resonance spectroscopy (MRS) prove to be beneficial. Nevertheless, the characteristics observed through radiology change as the disease advances. Different radiological criteria may be needed across different stages of the disease. This study aimed to assess the radiological characteristics of MSA-C or SCA 2 patients across various stages of the disease and to identify potential distinguishing factors.
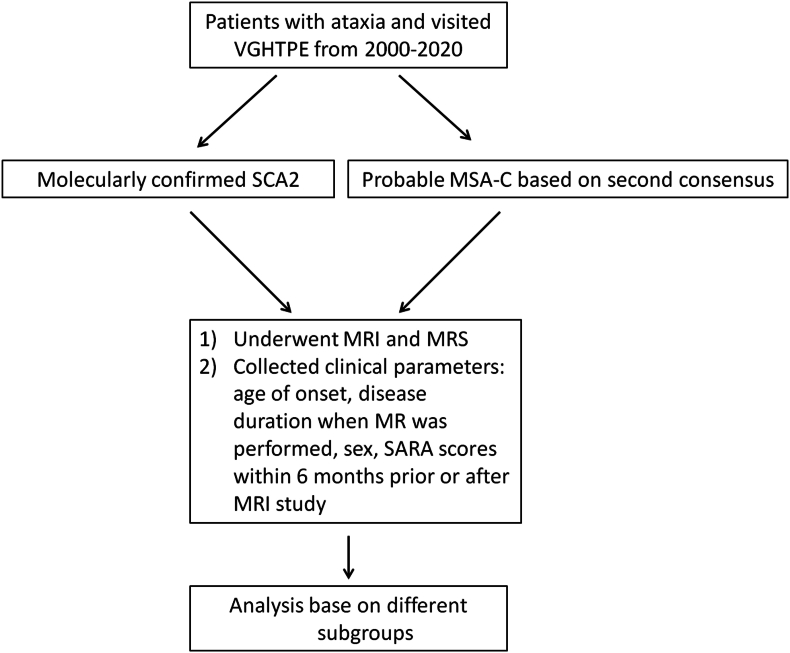
Methods: Between January 2000 and January 2020, a total of 390 patients, diagnosed with probable MSA-C according to the second consensus on MSA (317 cases) or with molecularly confirmed SCA 2 (73 cases), who had undergone at least one brain MRI and MRS targeting the cerebellar hemispheres, were enrolled in the study. The clinical parameters and neuroimaging features between these two diseases were compared and analyzed.
Results: A greater occurrence of a pontine hot cross bun sign (HCBS), higher scores on the scale for the assessment and rating of ataxia, and reduced levels of cerebellar N-acetyl aspartate (NAA)/creatine (Cr), and cerebellar choline (Cho)/Cr were found in MSA-C patients as compared with SCA 2 patients at similar disease durations. For the patients with an HCBS, a cerebellar Cho/Cr level of <0.53 was indicative of the potential presence of MSA-C, with significant level of specificity (85.96%).
Discussion: Discerning SCA2 from MSA-C using MRI and MRS appears to be plausible at various disease stages.
Keywords: HCBS; MRI; MRS; MSA-C; SCA2.
© 2024 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Bing-wen Soong reports financial support was provided by 10.13039/100020595Ministry of Science and Technology (MOST 107-2314-B-010-017 & MOST 107-2314-B-038-111), Taiwan, Republic of China.
Figures





Similar articles
-
Radiological hints for differentiation of cerebellar multiple system atrophy from spinocerebellar ataxia.Sci Rep. 2022 Jun 22;12(1):10499. doi: 10.1038/s41598-022-14531-0. Sci Rep. 2022. PMID: 35732792 Free PMC article.
-
Differences between spinocerebellar ataxias and multiple system atrophy-cerebellar type on proton magnetic resonance spectroscopy.PLoS One. 2012;7(10):e47925. doi: 10.1371/journal.pone.0047925. Epub 2012 Oct 31. PLoS One. 2012. PMID: 23118909 Free PMC article.
-
The merit of proton magnetic resonance spectroscopy in the longitudinal assessment of spinocerebellar ataxias and multiple system atrophy-cerebellar type.Cerebellum Ataxias. 2014 Dec 1;1:17. doi: 10.1186/s40673-014-0017-4. eCollection 2014. Cerebellum Ataxias. 2014. PMID: 26331041 Free PMC article.
-
The "Hot Cross Bun Sign" in Spinocerebellar Ataxia Types 2 and 7-Case Reports and Review of Literature.Mov Disord Clin Pract. 2022 Oct 13;9(8):1105-1113. doi: 10.1002/mdc3.13550. eCollection 2022 Nov. Mov Disord Clin Pract. 2022. PMID: 36339304 Free PMC article. Review.
-
Neurochemical profiles in hereditary ataxias: A meta-analysis of Magnetic Resonance Spectroscopy studies.Neurosci Biobehav Rev. 2020 Jan;108:854-865. doi: 10.1016/j.neubiorev.2019.12.019. Epub 2019 Dec 12. Neurosci Biobehav Rev. 2020. PMID: 31838195 Review.
Cited by
-
Exosomes in Regulating miRNAs for Biomarkers of Neurodegenerative Disorders.Mol Neurobiol. 2025 Jun;62(6):7576-7596. doi: 10.1007/s12035-025-04733-8. Epub 2025 Feb 7. Mol Neurobiol. 2025. PMID: 39918711 Review.
References
-
- Lin D.J., Hermann K.L., Schmahmann J.D. Multiple system atrophy of the cerebellar type: clinical state of the art. Mov. Disord. 2014;29(3):294–304. - PubMed
-
- Gilman S., Wenning G.K., Low P.A., Brooks D.J., Mathias C.J., Trojanowski J.Q., Wood N.W., Colosimo C., Durr A., Fowler C.J., Kaufmann H., Klockgether T., Lees A., Poewe W., Quinn N., Revesz T., Robertson D., Sandroni P., Seppi K., Vidailhet M. Second consensus statement on the diagnosis of multiple system atrophy. Neurology. 2008;71(9):670–676. - PMC - PubMed
-
- Kim H.J., Stamelou M., Jeon B. Multiple system atrophy-mimicking conditions: diagnostic challenges. Parkinsonism Relat. Disorders. 2016;22(Suppl 1):S12–S15. - PubMed
-
- Lastres-Becker I., Rub U., Auburger G. Spinocerebellar ataxia 2 (SCA2) Cerebellum. 2008;7(2):115–124. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
