

Polygenic risk and incident coronary heart disease in a large multiethnic cohort
- PMID: 38601895
- PMCID: PMC11004687
- DOI: 10.1016/j.ajpc.2024.100661
Polygenic risk and incident coronary heart disease in a large multiethnic cohort
Abstract
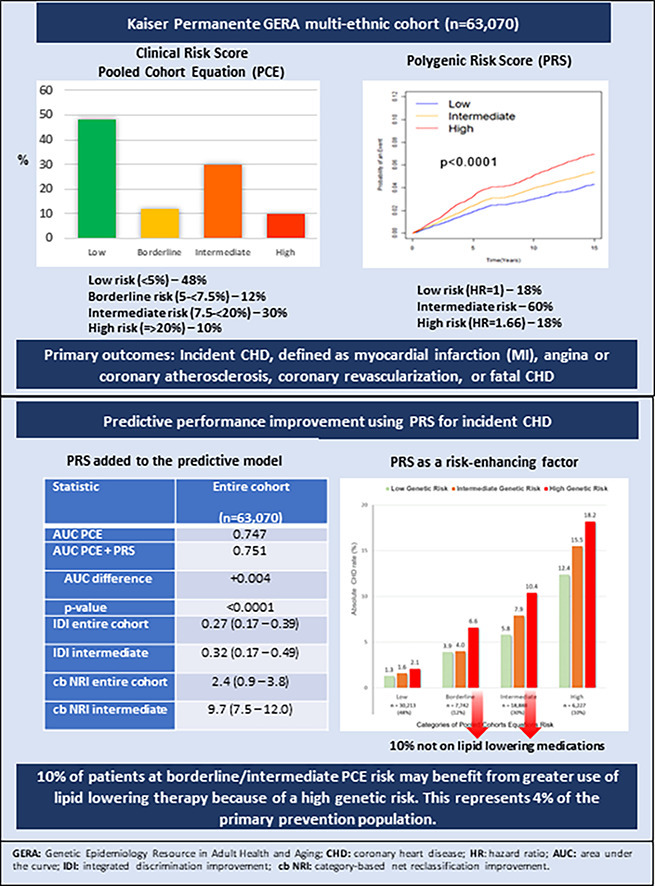
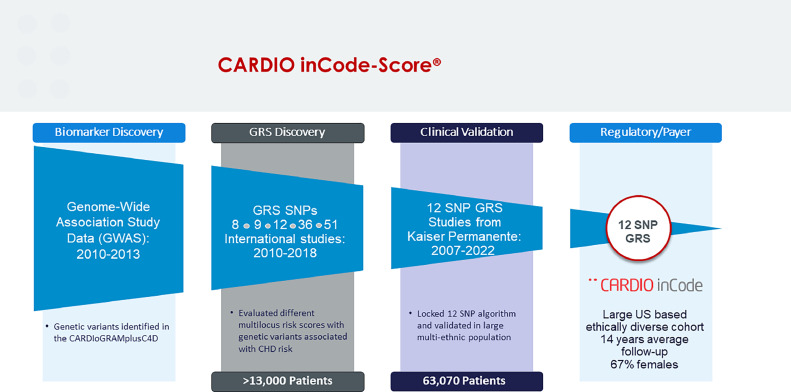
Objective: Many studies support the notion that polygenic risk scores (PRS) improve risk prediction for coronary heart disease (CHD) beyond conventional risk factors. However, PRS are not yet considered risk-enhancing factor in guidelines. Our objective was to determine the predictive performance of a commercially available PRS (CARDIO inCode-Score®) compared with the Pooled Cohorts Equations (PCE) in a contemporary, multi-ethnic cohort.
Methods: Participants (n = 63,070; 67 % female; 18 % non-European) without prior CHD were followed from 2007 through 12/31/2022. The association between the PRS and incident CHD was assessed using Cox regression adjusting for genetic ancestry and risk factors. Event rates were estimated by categories of PCE and by low/intermediate/high genetic risk within PCE categories; risk discrimination and net reclassification improvement (NRI) were also assessed.
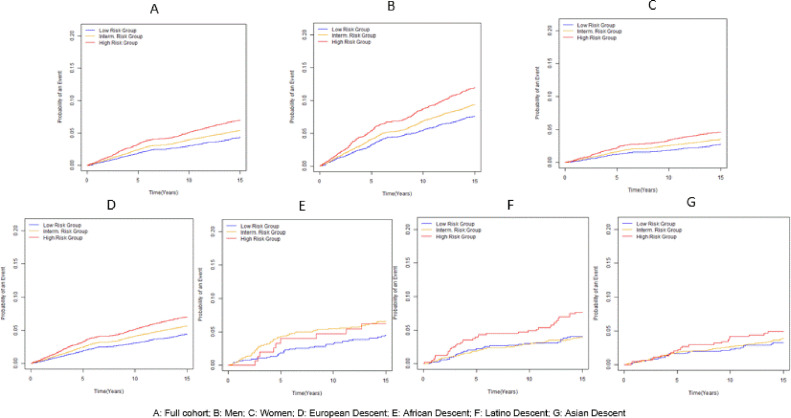
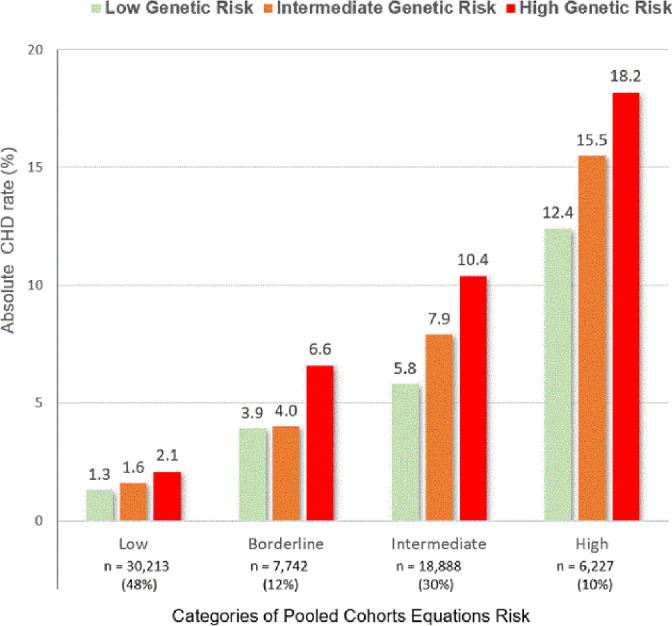
Results: There were 3,289 incident CHD events during 14 years of follow-up. Adjusted hazard ratio (aHR) for incident CHD per 1 SD increase in PRS was 1.18 (95 % CI:1.14-1.22), and the aHR for the upper vs lower quintile of the PRS was 1.66 (95 % CI:1.49-1.86). The association was consistent in both sexes, in European participants compared with all minority groups combined and was strongest in the first 5 years of follow-up. The increase in the C-statistic was 0.004 (0.747 vs. 0.751; p < 0.0001); the NRI was 2.4 (0.9-3.8) for the entire cohort and 9.7 (7.5-12.0) for intermediate PCE risk individuals. After incorporating high genetic risk, a further 10 percent of participants at borderline/intermediate PCE risk would be candidates for statin therapy.
Conclusion: Inclusion of polygenic risk improved identification of primary prevention individuals who may benefit from more intensive risk factor modification.
Keywords: Clinical utility; Coronary heart disease; Polygenic risk score; Primary prevention.
© 2024 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Carlos Iribarren reports financial support was provided by GENinCode, Plc. Roberto Elosua is a member of the scientific advisory board of GENinCode, Plc, and inventor in a patent application based on the CARDIOinCODE-Score® CHD PRS whose applicant is GENinCode, Plc. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Lloyd-Jones D.M., Braun L.T., Ndumele C.E., et al. Use of risk assessment tools to guide decision-making in the primary prevention of atherosclerotic cardiovascular disease: a special report from the american heart association and American college of cardiology. Circulation. 2019;139:e1162–e1177. - PubMed
