

Multimodal automatic assessment of acute pain through facial videos and heart rate signals utilizing transformer-based architectures
- PMID: 38601923
- PMCID: PMC11004333
- DOI: 10.3389/fpain.2024.1372814
Multimodal automatic assessment of acute pain through facial videos and heart rate signals utilizing transformer-based architectures
Abstract
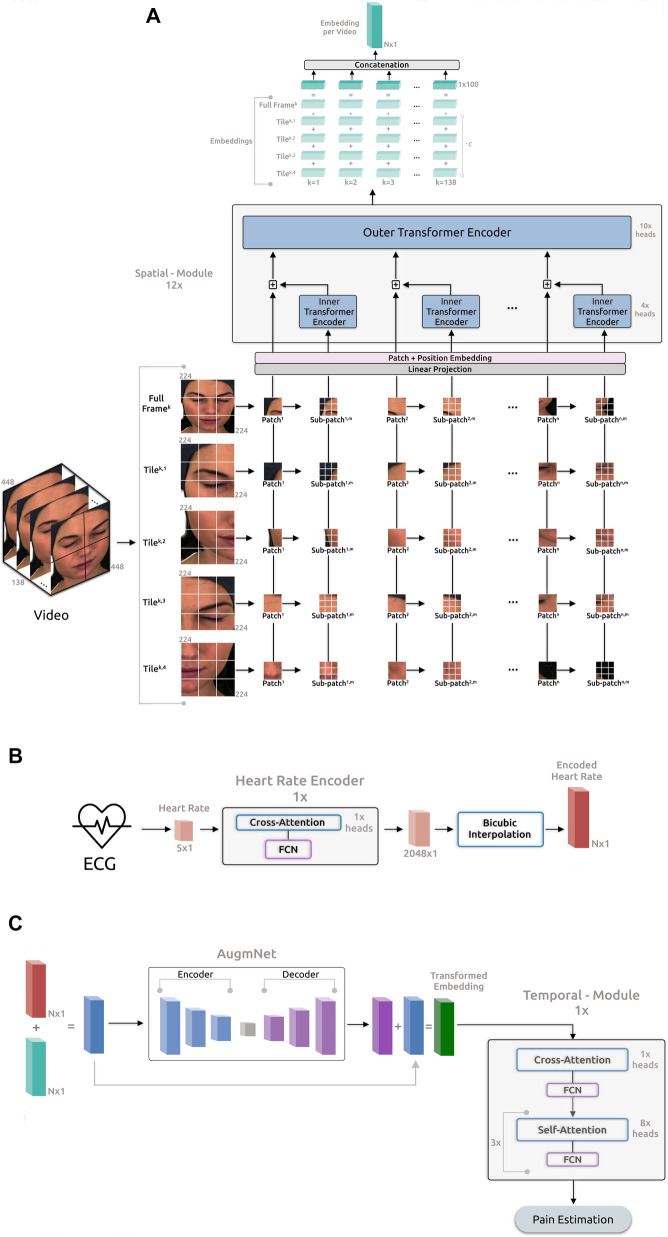
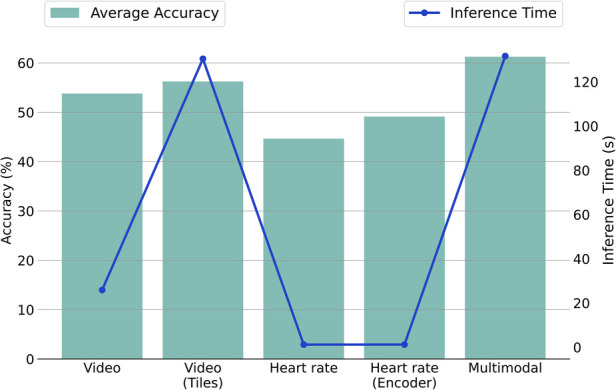
Accurate and objective pain evaluation is crucial in developing effective pain management protocols, aiming to alleviate distress and prevent patients from experiencing decreased functionality. A multimodal automatic assessment framework for acute pain utilizing video and heart rate signals is introduced in this study. The proposed framework comprises four pivotal modules: the Spatial Module, responsible for extracting embeddings from videos; the Heart Rate Encoder, tasked with mapping heart rate signals into a higher dimensional space; the AugmNet, designed to create learning-based augmentations in the latent space; and the Temporal Module, which utilizes the extracted video and heart rate embeddings for the final assessment. The Spatial-Module undergoes pre-training on a two-stage strategy: first, with a face recognition objective learning universal facial features, and second, with an emotion recognition objective in a multitask learning approach, enabling the extraction of high-quality embeddings for the automatic pain assessment. Experiments with the facial videos and heart rate extracted from electrocardiograms of the BioVid database, along with a direct comparison to 29 studies, demonstrate state-of-the-art performances in unimodal and multimodal settings, maintaining high efficiency. Within the multimodal context, 82.74% and 39.77% accuracy were achieved for the binary and multi-level pain classification task, respectively, utilizing million parameters for the entire framework.
Keywords: ECG; data fusion; deep learning; pain recognition; vision transformer.
© 2024 Gkikas, Tachos, Andreadis, Pezoulas, Zaridis, Gkois, Matonaki, Stavropoulos and Fotiadis.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
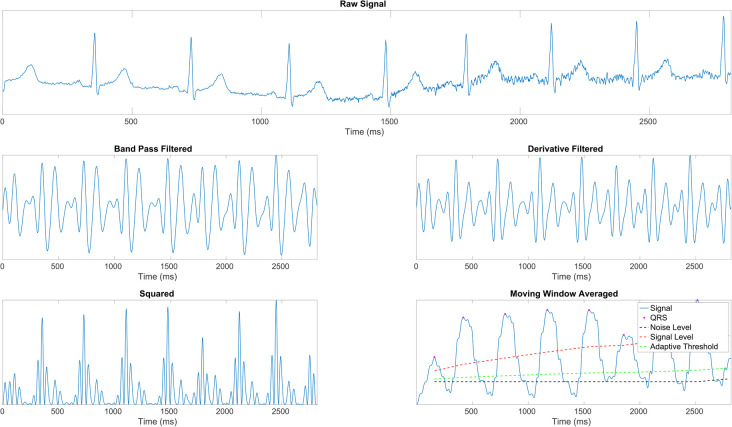
 ) with identified R peaks (
) with identified R peaks ( ), noise level (– –), signal level (
), noise level (– –), signal level ( ), and adaptive thresholding (
), and adaptive thresholding ( ).
).
Similar articles
-
A Multimodal Pain Sentiment Analysis System Using Ensembled Deep Learning Approaches for IoT-Enabled Healthcare Framework.Sensors (Basel). 2025 Feb 17;25(4):1223. doi: 10.3390/s25041223. Sensors (Basel). 2025. PMID: 40006452 Free PMC article.
-
SMaTE: A Segment-Level Feature Mixing and Temporal Encoding Framework for Facial Expression Recognition.Sensors (Basel). 2022 Aug 1;22(15):5753. doi: 10.3390/s22155753. Sensors (Basel). 2022. PMID: 35957313 Free PMC article.
-
A Comprehensive Study on Pain Assessment from Multimodal Sensor Data.Sensors (Basel). 2023 Dec 7;23(24):9675. doi: 10.3390/s23249675. Sensors (Basel). 2023. PMID: 38139521 Free PMC article.
-
Multi-speed transformer network for neurodegenerative disease assessment and activity recognition.Comput Methods Programs Biomed. 2023 Mar;230:107344. doi: 10.1016/j.cmpb.2023.107344. Epub 2023 Jan 9. Comput Methods Programs Biomed. 2023. PMID: 36706617
-
A Full Transformer-based Framework for Automatic Pain Estimation using Videos.Annu Int Conf IEEE Eng Med Biol Soc. 2023 Jul;2023:1-6. doi: 10.1109/EMBC40787.2023.10340872. Annu Int Conf IEEE Eng Med Biol Soc. 2023. PMID: 38083481
Cited by
-
Facial expression deep learning algorithms in the detection of neurological disorders: a systematic review and meta-analysis.Biomed Eng Online. 2025 May 22;24(1):64. doi: 10.1186/s12938-025-01396-3. Biomed Eng Online. 2025. PMID: 40405223 Free PMC article.
-
Pseudo-labeling based adaptations of pain domain classifiers.Front Pain Res (Lausanne). 2025 Apr 23;6:1562099. doi: 10.3389/fpain.2025.1562099. eCollection 2025. Front Pain Res (Lausanne). 2025. PMID: 40337527 Free PMC article.
-
Expert consensus on feasibility and application of automatic pain assessment in routine clinical use.J Anesth Analg Crit Care. 2025 Jun 2;5(1):29. doi: 10.1186/s44158-025-00249-8. J Anesth Analg Crit Care. 2025. PMID: 40457422 Free PMC article. Review.
-
Dual stream transformer for medication state classification in Parkinson's disease patients using facial videos.NPJ Digit Med. 2025 Apr 26;8(1):226. doi: 10.1038/s41746-025-01630-1. NPJ Digit Med. 2025. PMID: 40287603 Free PMC article.
-
A CrossMod-Transformer deep learning framework for multi-modal pain detection through EDA and ECG fusion.Sci Rep. 2025 Aug 12;15(1):29467. doi: 10.1038/s41598-025-14238-y. Sci Rep. 2025. PMID: 40796769 Free PMC article.
References
-
- Turk DC, Melzack R. The measurement of pain, the assessment of people experiencing pain. In: Handbook of Pain Assessment. The Guilford Press (2011). p. 3–16.
-
- De Ruddere L, Tait R. Facing Others in Pain: Why Context Matters. Cham: Springer International Publishing; (2018). p. 241–69.
LinkOut - more resources
Full Text Sources