

Comparing the outcomes and costs of cardiac monitoring with implantable loop recorders and mobile cardiac outpatient telemetry following stroke using real-world evidence
- PMID: 38602503
- PMCID: PMC11145532
- DOI: 10.57264/cer-2024-0008
Comparing the outcomes and costs of cardiac monitoring with implantable loop recorders and mobile cardiac outpatient telemetry following stroke using real-world evidence
Abstract
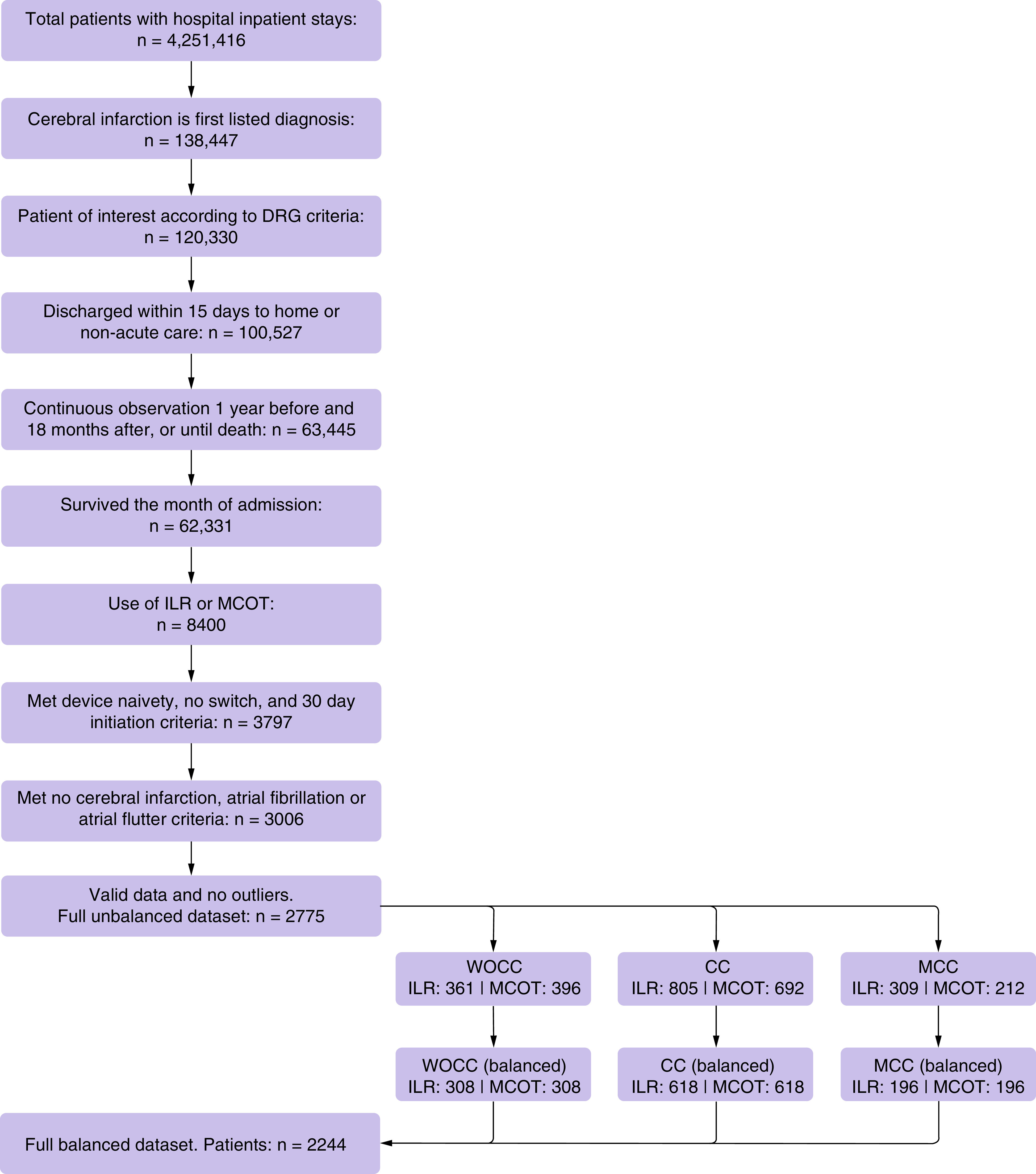
Aim: Patients with ischemic stroke (IS) commonly undergo monitoring to identify atrial fibrillation with mobile cardiac outpatient telemetry (MCOT) or implantable loop recorders (ILRs). The authors compared readmission, healthcare cost and survival in patients monitored post-stroke with either MCOT or ILR. Materials & methods: The authors used claims data from Optum's de-identified Clinformatics® Data Mart Database to identify patients with IS hospitalized from January 2017 to December 2020 who were prescribed ambulatory cardiac monitoring via MCOT or ILR. They compared the costs associated with the initial inpatient visit as well as the rate and causes of readmission, survival and healthcare costs over the following 18 months. Datasets were balanced using patient baseline and hospitalization characteristics. Multivariable generalized linear gamma regression was used for cost comparisons. Cox proportional hazard regression was used for survival and readmission analysis. Sub-cohorts were analyzed based on the severity of the index IS. Results: In 2244 patients, readmissions were significantly lower in the MCOT monitored group (30.2%) compared with the ILR group (35.4%) (hazard ratio [HR] 1.23; 95% CI: 1.04-1.46). Average cost over 18 months starting with the index IS was $27,429 (USD) lower in the MCOT group (95% CI: $22,353-$32,633). Survival difference bordered on statistical significance and trended to lower mortality in MCOT (8.9%) versus ILR (11.3%) (HR 1.30; 95% CI: 1:00-1.69), led by significance in patients with complications or comorbidities with the index event (MCOT 7.5%, ILR 11.5%; HR 1.62; 95% CI: 1.11-2.36). Conclusion: The use of MCOT versus ILR as the primary monitor following IS was associated with significant decreases in readmission, lower costs for the initial IS and total care over the next 18 months, significantly lower mortality for patients with complications and comorbidities at the index stroke, and a trend toward improved survival across all patients.
Keywords: ICM; ILR; MCOT; MCT; costs; cryptogenic stroke; health economics; healthcare costs; implantable loop recorder; ischemic stroke; mobile cardiac outpatient telemetry; mortality; readmissions; real-world evidence; stroke.
Conflict of interest statement
Competing interests disclosure
G Medic, A Dunn, R Vazquez and V Norlock are the employees of Philips. Philips is a producer of MCOT. M Kyriakakos and C Siegfried are employees of Veranex. Veranex received funding from Philips to write the manuscript. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures

Similar articles
-
Mobile Cardiac Outpatient Telemetry Patch vs Implantable Loop Recorder in Cryptogenic Stroke Patients in the US - Cost-Minimization Model.Med Devices (Auckl). 2021 Dec 18;14:445-458. doi: 10.2147/MDER.S337142. eCollection 2021. Med Devices (Auckl). 2021. PMID: 34955658 Free PMC article.
-
Effectiveness, utilisation and cost associated with implantable loop recorders versus external monitors after ischaemic or cryptogenic stroke.Open Heart. 2024 May 8;11(1):e002714. doi: 10.1136/openhrt-2024-002714. Open Heart. 2024. PMID: 38719499 Free PMC article.
-
A meta-analysis of extended ECG monitoring in detection of atrial fibrillation in patients with cryptogenic stroke.Open Heart. 2022 Sep;9(2):e002081. doi: 10.1136/openhrt-2022-002081. Open Heart. 2022. PMID: 36175044 Free PMC article.
-
Outpatient cardiac telemetry detects a high rate of atrial fibrillation in cryptogenic stroke.J Neurol Sci. 2013 Jan 15;324(1-2):57-61. doi: 10.1016/j.jns.2012.10.001. Epub 2012 Oct 24. J Neurol Sci. 2013. PMID: 23102659
-
ECG Smart Monitoring versus Implantable Loop Recorders for Atrial Fibrillation Detection after Cryptogenic Stroke-An Overview for Decision Making.J Cardiovasc Dev Dis. 2023 Jul 18;10(7):306. doi: 10.3390/jcdd10070306. J Cardiovasc Dev Dis. 2023. PMID: 37504563 Free PMC article. Review.
Cited by
-
A hybrid cardiovascular arrhythmia disease detection using ConvNeXt-X models on electrocardiogram signals.Sci Rep. 2024 Dec 5;14(1):30366. doi: 10.1038/s41598-024-81992-w. Sci Rep. 2024. PMID: 39638880 Free PMC article.
References
-
- Tsao CW, Aday AW, Almarzooq ZI et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics – 2023 Update: a report from the American Heart Association. Circulation 147(8), e93–e621 (2023). - PubMed
-
- Martin SS, Aday AW, Almarzooq ZI et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. 2024 Heart Disease and Stroke Statistics: a report of US and global data from the American Heart Association. Circulation 149(8), e347–e913 (2024). - PubMed
-
- Moraes MA, Jesus PAP, Muniz LS et al. Mortalidade por acidente vascular cerebral isquêmico e tempo de chegada a hospital: análise dos primeiros 90 dias. Rev. Esc. Enferm. USP 57, e20220309 (2023). - PubMed
-
- Cardiogenic brain embolism. The second report of the Cerebral Embolism Task Force. Arch. Neurol. 46(7), 727–743 (1989). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources