

Parkinson's disease and vitamins: a focus on vitamin B12
- PMID: 38602571
- PMCID: PMC11608379
- DOI: 10.1007/s00702-024-02769-z
Parkinson's disease and vitamins: a focus on vitamin B12
Abstract
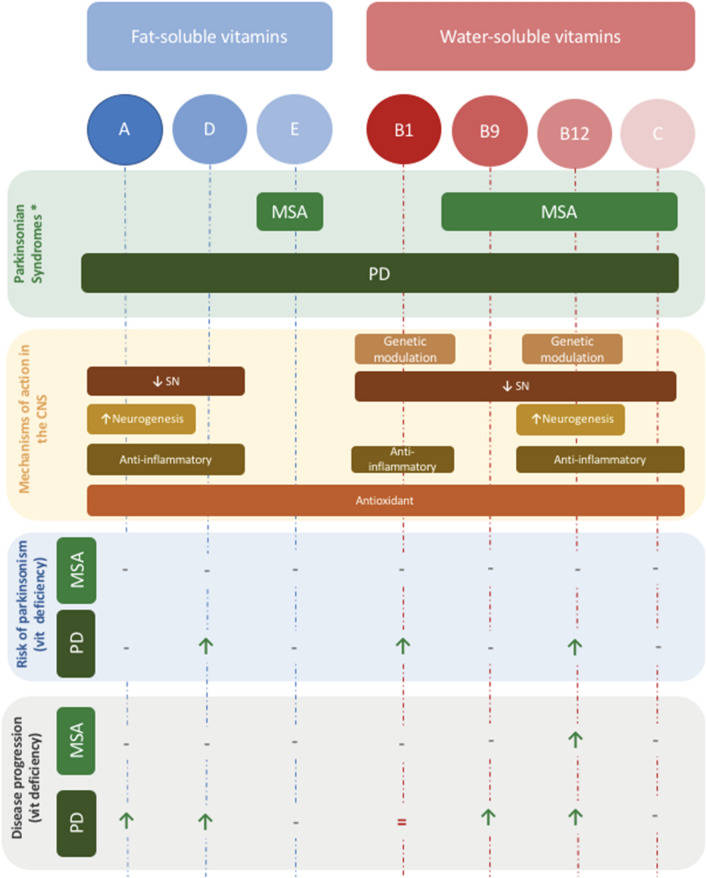
Parkinson's disease (PD) has been linked to a vast array of vitamins among which vitamin B12 (Vit B12) is the most relevant and often investigated specially in the context of intrajejunal levodopa infusion therapy. Vit B12 deficiency, itself, has been reported to cause acute parkinsonism. Nevertheless, concrete mechanisms through which B12 deficiency interacts with PD in terms of pathophysiology, clinical manifestation and progression remains unclear. Recent studies have suggested that Vit B12 deficiency along with the induced hyperhomocysteinemia are correlated with specific PD phenotypes characterized with early postural instability and falls and more rapid motor progression, cognitive impairment, visual hallucinations and autonomic dysfunction. Specific clinical features such as polyneuropathy have also been linked to Vit B12 deficiency specifically in context of intrajejunal levodopa therapy. In this review, we explore the link between Vit B12 and PD in terms of physiopathology regarding dysfunctional neural pathways, neuropathological processes as well as reviewing the major clinical traits of Vit B12 deficiency in PD and Levodopa-mediated neuropathy. Finally, we provide an overview of the therapeutic effect of Vit B12 supplementation in PD and posit a practical guideline for Vit B12 testing and supplementation.
Keywords: Homocysteine; Motor; Non-motor; Parkinson’s disease; Vitamin B12; Vitamins.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: All authors declare no financial or non-financial competing interests.
Figures




References
-
- Al Amin ASM, Gupta V (2023) Vitamin B12 (Cobalamin). In: StatPearls. StatPearls Publishing, Treasure Island. https://www.ncbi.nlm.nih.gov/books/NBK559132/ - PubMed
-
- Andréasson M, Brodin L, Laffita-Mesa JM, Svenningsson P (2017) Correlations between methionine cycle metabolism, COMT genotype, and polyneuropathy in L-dopa treated Parkinson’s disease: a preliminary cross-sectional study. J Park Dis 7:619–628 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
