

Particle analysis of surgical lung biopsies from deployed and non-deployed US service members during the Global War on Terrorism
- PMID: 38603724
- PMCID: PMC11008878
- DOI: 10.1371/journal.pone.0301868
Particle analysis of surgical lung biopsies from deployed and non-deployed US service members during the Global War on Terrorism
Abstract
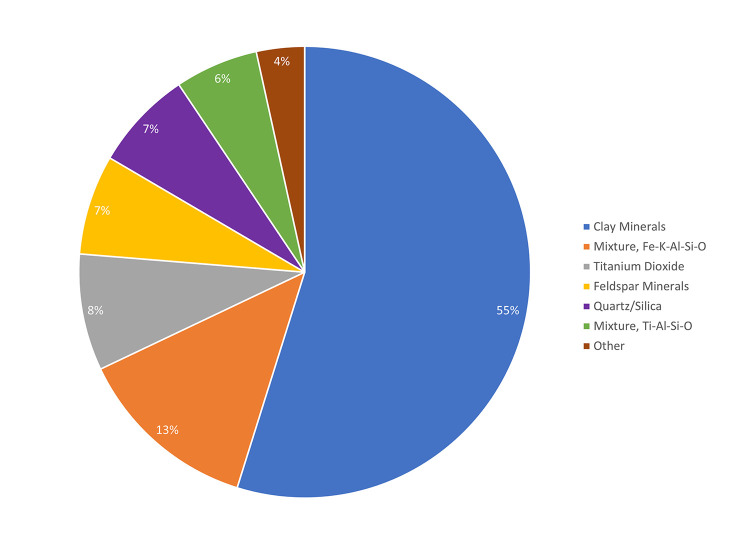
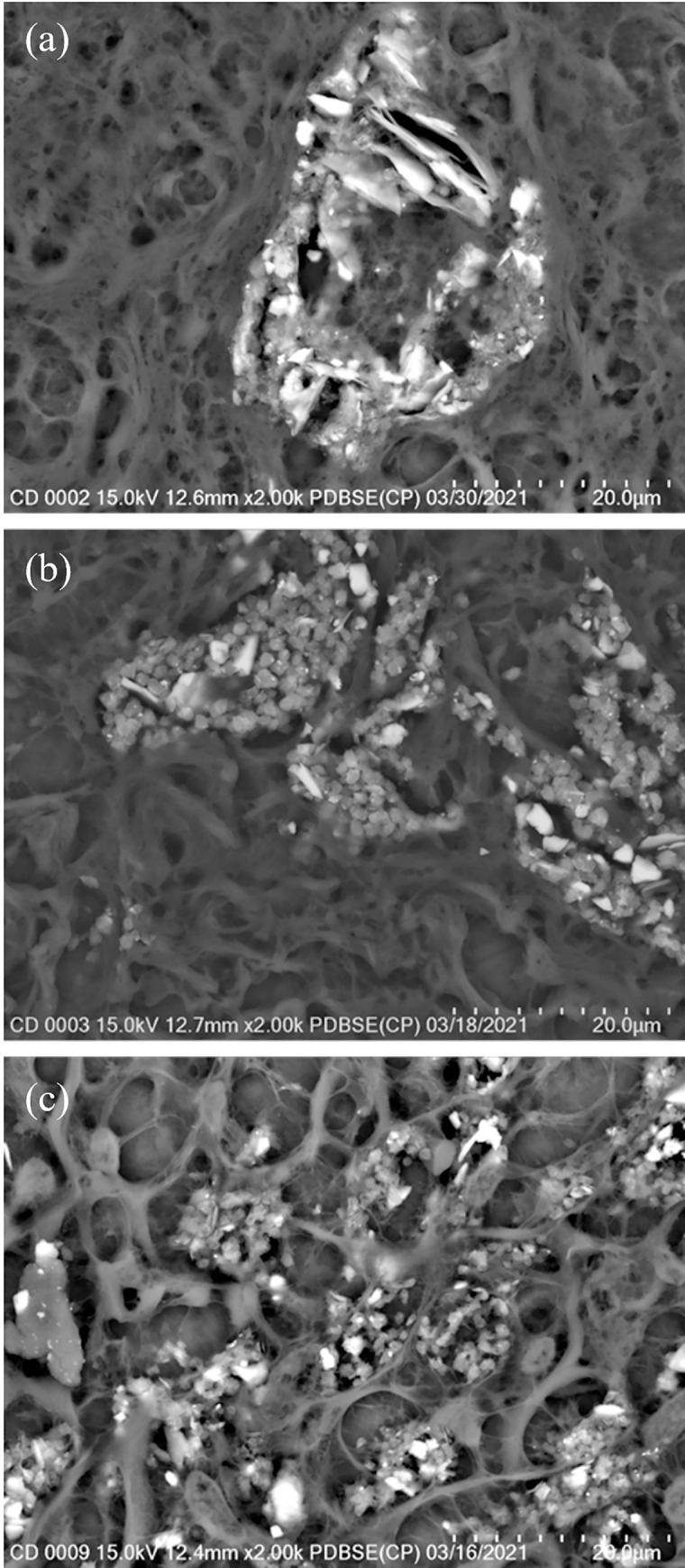
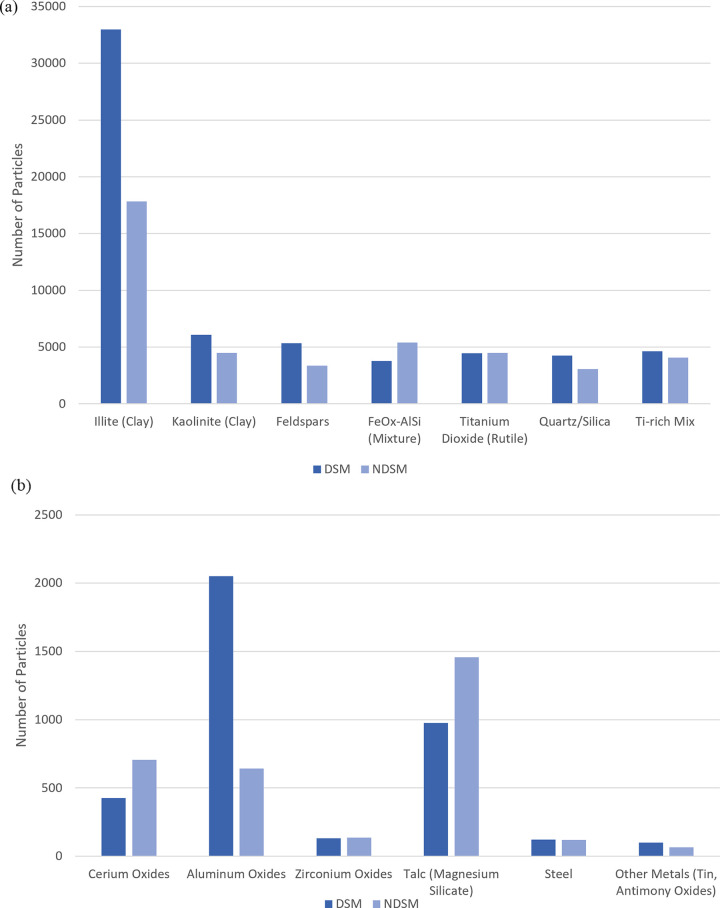
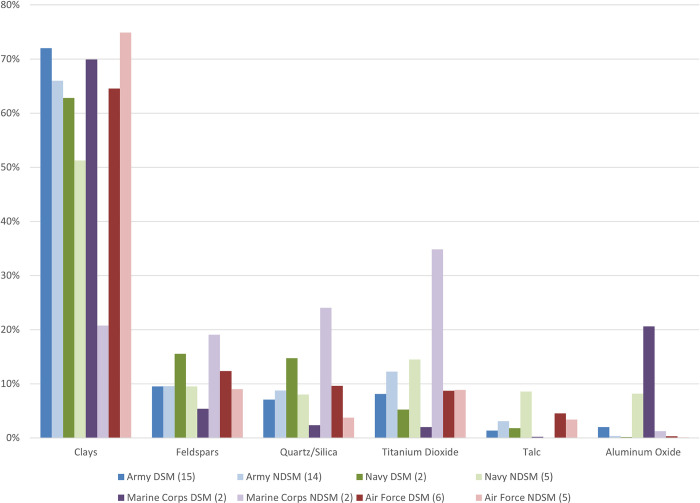
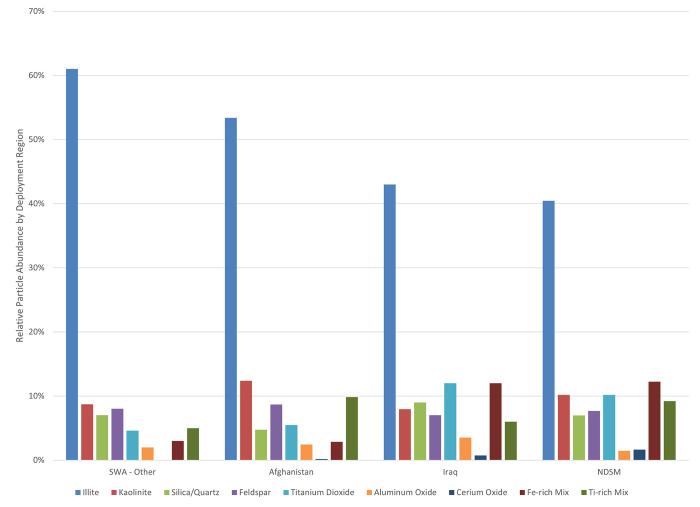
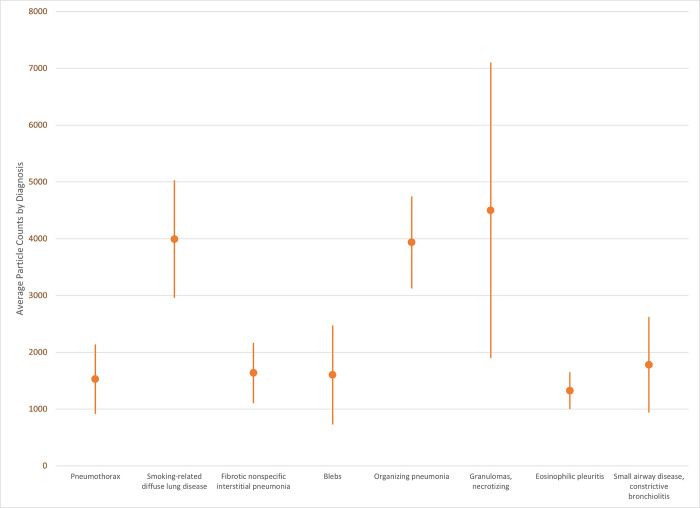
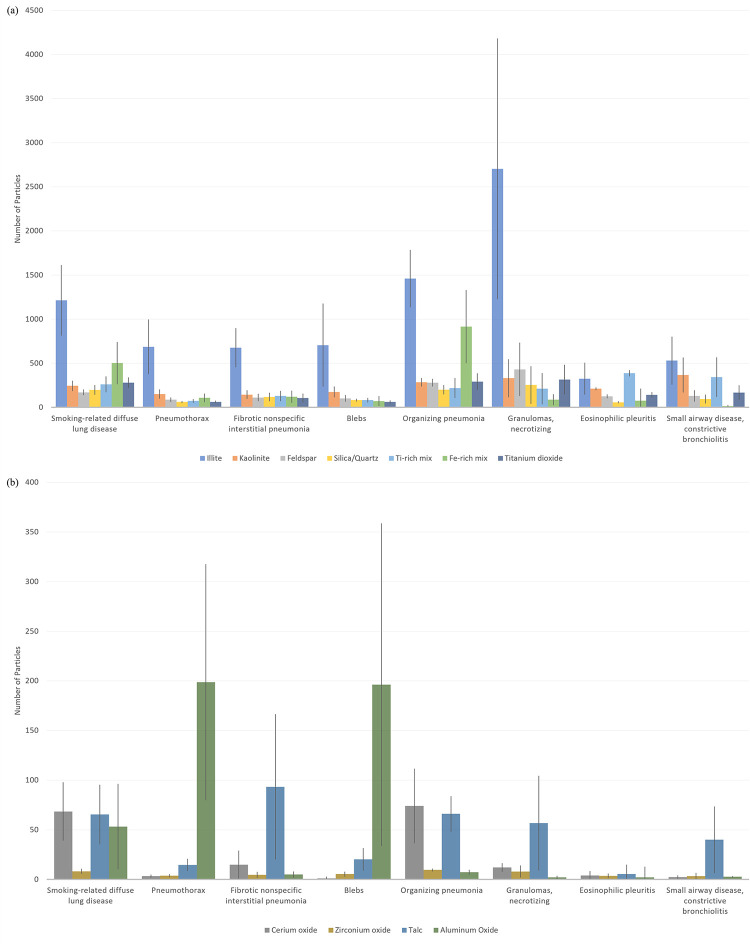
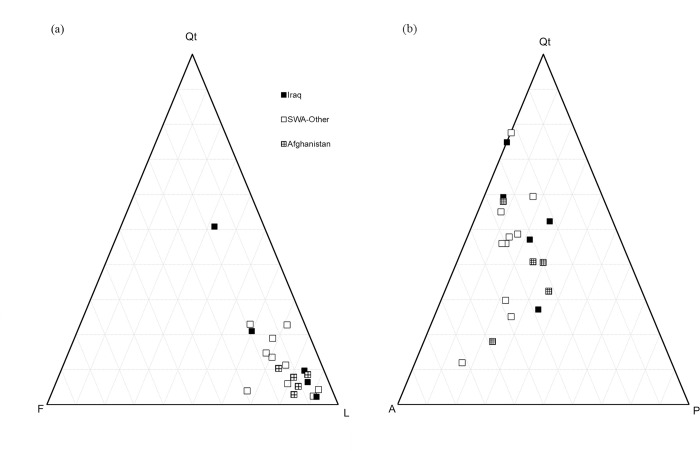
The role that inhaled particulate matter plays in the development of post-deployment lung disease among US service members deployed to Southwest Asia during the Global War on Terrorism has been difficult to define. There is a persistent gap in data addressing the relationship between relatively short-term (months to a few years) exposures to high levels of particulate matter during deployment and the subsequent development of adverse pulmonary outcomes. Surgical lung biopsies from deployed service members and veterans (DSMs) and non-deployed service members and veterans (NDSMs) who develop lung diseases can be analyzed to potentially identify residual deployment-specific particles and develop associations with pulmonary pathological diagnoses. We examined 52 surgical lung biopsies from 25 DSMs and 27 NDSMs using field emission scanning electron microscopy (FE-SEM) with energy dispersive x-ray spectroscopy (EDS) to identify any between-group differences in the number and composition of retained inorganic particles, then compared the particle analysis results with the original histopathologic diagnoses. We recorded a higher number of total particles in biopsies from DSMs than from NDSMs, and this difference was mainly accounted for by geologic clays (illite, kaolinite), feldspars, quartz/silica, and titanium-rich silicate mixtures. Biopsies from DSMs deployed to other Southwest Asia regions (SWA-Other) had higher particle counts than those from DSMs primarily deployed to Iraq or Afghanistan, due mainly to illite. Distinct deployment-specific particles were not identified. Particles did not qualitatively associate with country of deployment. The individual diagnoses of the DSMs and NDSMs were not associated with elevated levels of total particles, metals, cerium oxide, or titanium dioxide particles. These results support the examination of particle-related lung disease in DSMs in the context of comparison groups, such as NDSMs, to assist in determining the strength of associations between specific pulmonary pathology diagnoses and deployment-specific inorganic particulate matter exposure.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Particle Analysis by Scanning Electron Microscopy With Energy Dispersive X-Ray Analysis in Pulmonary Pathology Specimens From U.S. Military Service Members Deployed During the Global War on Terror 2002 to 2015.Mil Med. 2021 Jan 25;186(Suppl 1):784-788. doi: 10.1093/milmed/usaa318. Mil Med. 2021. PMID: 33499496
-
Pulmonary Pathology Diagnoses in the US Military During the Global War on Terrorism.Lung. 2021 Aug;199(4):345-355. doi: 10.1007/s00408-021-00446-6. Epub 2021 Aug 7. Lung. 2021. PMID: 34363506 Review.
-
Iraq/Afghanistan war lung injury reflects burn pits exposure.Sci Rep. 2022 Aug 29;12(1):14671. doi: 10.1038/s41598-022-18252-2. Sci Rep. 2022. PMID: 36038588 Free PMC article.
-
Method to characterize inorganic particulates in lung tissue biopsies using field emission scanning electron microscopy.Toxicol Mech Methods. 2018 Sep;28(7):475-487. doi: 10.1080/15376516.2018.1449042. Epub 2018 Apr 23. Toxicol Mech Methods. 2018. PMID: 29685079
-
Role of Particulate Matter from Afghanistan and Iraq in Deployment-Related Lung Disease.Chem Res Toxicol. 2021 Dec 20;34(12):2408-2423. doi: 10.1021/acs.chemrestox.1c00090. Epub 2021 Nov 22. Chem Res Toxicol. 2021. PMID: 34808040 Review.
Cited by
-
Current understanding of the impact of United States military airborne hazards and burn pit exposures on respiratory health.Part Fibre Toxicol. 2024 Oct 21;21(1):43. doi: 10.1186/s12989-024-00606-5. Part Fibre Toxicol. 2024. PMID: 39434148 Free PMC article. Review.
References
-
- Defense Manpower Data Center, Monterey CA. Lewin-Smith M. Personal communication. December 2022.
-
- Wenger JW O’Connell C, Cottrell L. Examination of recent deployment experience across the services and components. Santa Monica, CA: Rand Corporation; 2018.
-
- Institute of Medicine. Long-term health consequences of exposure to burn pits in Iraq and Afghanistan. Washington, DC: National Academies Press; 2011.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
