

Enhancing NSCLC recurrence prediction with PET/CT habitat imaging, ctDNA, and integrative radiogenomics-blood insights
- PMID: 38605064
- PMCID: PMC11009351
- DOI: 10.1038/s41467-024-47512-0
Enhancing NSCLC recurrence prediction with PET/CT habitat imaging, ctDNA, and integrative radiogenomics-blood insights
Abstract
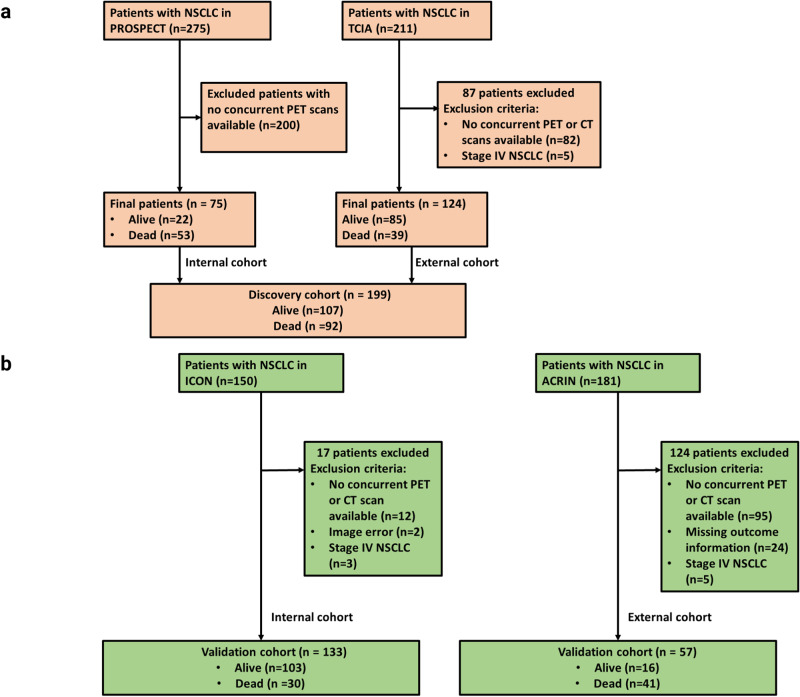
While we recognize the prognostic importance of clinicopathological measures and circulating tumor DNA (ctDNA), the independent contribution of quantitative image markers to prognosis in non-small cell lung cancer (NSCLC) remains underexplored. In our multi-institutional study of 394 NSCLC patients, we utilize pre-treatment computed tomography (CT) and 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) to establish a habitat imaging framework for assessing regional heterogeneity within individual tumors. This framework identifies three PET/CT subtypes, which maintain prognostic value after adjusting for clinicopathologic risk factors including tumor volume. Additionally, these subtypes complement ctDNA in predicting disease recurrence. Radiogenomics analysis unveil the molecular underpinnings of these imaging subtypes, highlighting downregulation in interferon alpha and gamma pathways in the high-risk subtype. In summary, our study demonstrates that these habitat imaging subtypes effectively stratify NSCLC patients based on their risk levels for disease recurrence after initial curative surgery or radiotherapy, providing valuable insights for personalized treatment approaches.
© 2024. The Author(s).
Conflict of interest statement
X.L. reports Consulting/advisory fees from Eli Lilly, EMD Serono (Merck KGaA), AstraZeneca, Spectrum Pharmaceutics, Novartis, Regeneron, Boehringer Ingelheim, Hengrui Therapeutics, Bayer, Teligene, Taiho, Daiichi Sankyo, Janssen, Blueprint Medicines, Sensei Biotherapeutics, SystImmune, ArriVent, Abion, and Abbvie Research Funding to Institution from Eli Lilly, EMD Serono, ArriVent, Dizal, Teligene, Regeneron, Janssen, ThermoFisher, Takeda, and Boehringer Ingelheim. Travel Support from EMD Serono, Janssen, and Spectrum Pharmaceutics. Stock options from BlossomHill. T.C. reports speaker fees and honoraria from The Society for Immunotherapy of Cancer, Bristol Myers Squibb, Roche, Medscape, and PeerView; having an advisory role or receiving consulting fees from AstraZeneca, Bristol Myers Squibb, EMD Serono, Merck & Co, Genentech, and Arrowhead Pharmaceuticals; and institutional research funding from AstraZeneca, Bristol Myers Squibb, and EMD Serono. N.I.V. receives consulting fees from Sanofi, Regeneron, Oncocyte, and Eli Lilly; and research funding from Mirati outside the submitted work. J.Y.C. reports research funding from BMS-MDACC, Siemens Healthcare, and consultation fees from Legion Healthcare Partners. L.Y. has grant support from Lantheus Inc. M.C.B.G. has received research funding from Siemens Healthcare. I.W. has received honoraria from Genentech/Roche, Astra Zeneca, Merck, Guardant Health, Flame, Novartis, Sanofi, Daiichi Sankyo, Dava Oncology, Amgen, GlaxoSmithKline, HTG Molecular, Jansen, Merus, Imagene, G1 Therapeutics, Abbvie, Catalyst Therapeutics, Genzyme, Regeneron, Oncocyte, Medscape, Platform Health, Pfizer, Physicians’ Education Resource, HPM Education, and Aptitute Health; Additionally, I.W. has received research support from Genentech, Merck, Bristol-Myers Squibb, Medimmune, Adaptive, Adaptimmune, EMD Serono, Pfizer, Takeda, Amgen, Karus, Johnson & Johnson, Bayer, Iovance, 4D, Novartis, and Akoya. D.L.G. has served on scientific advisory committees for Menarini Ricerche, 4D Pharma, Onconova, and Eli Lilly and has received research support from Takeda, Astellas, NGM Biopharmaceuticals, Boehringer Ingelheim and AstraZeneca. J.V.H. reports being on scientific advisory boards for AstraZeneca, Boehringer Ingelheim, Genentech, GlaxoSmithKline, Eli Lilly, Novartis, Spectrum, EMD Serono, Sanofi, Takeda, Mirati Therapeutics, BMS, and Janssen Global Services; receiving research support from AstraZeneca, Takeda, Boehringer Ingelheim, and Spectrum; and receiving licensing fees from Spectrum. C.C.W reports research support from the Medical Imaging and Data Resource Center from NIBIB/University of Chicago and royalties from Elsevier. J.Z. reports serving on the consulting/advisory board of Bristol-Myers Squibb, AstraZeneca, Novartis, Johnson & Johnson, GenePlus, Innovent, Varian, and Catalyst; receiving research grants to institutions from Merck, Novartis, and Johnson & Johnson. J.W. reports research funding from Siemens Healthcare. The remaining authors declare no competing interests.
Figures





References
-
- Vaidya P, et al. CT derived radiomic score for predicting the added benefit of adjuvant chemotherapy following surgery in stage I, II resectable non-small cell lung cancer: a retrospective multicohort study for outcome prediction. Lancet Digital Health. 2020;2:e116–e128. doi: 10.1016/S2589-7500(20)30002-9. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
