

The timing of minimally invasive surgery for prenatally diagnosed choledochal cysts
- PMID: 38605324
- PMCID: PMC11010284
- DOI: 10.1186/s12887-024-04734-x
The timing of minimally invasive surgery for prenatally diagnosed choledochal cysts
Abstract
Objective: There are no clear evidence-based recommendations concerning when patients with prenatally diagnosed choledochal cysts (CCs) should undergo surgery. This study was primarily designed to explore the proper timing of minimally invasive surgery for prenatally diagnosed CC patients.
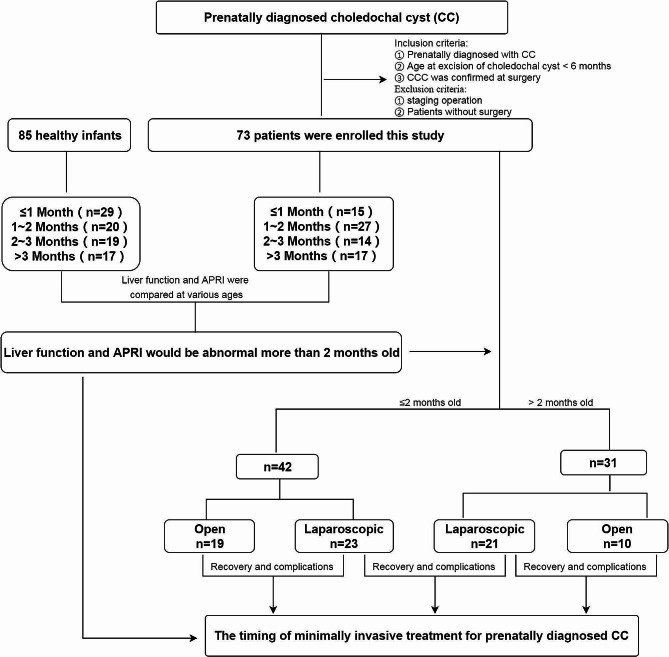
Methods: Seventy-three patients with prenatally diagnosed CC were enrolled in this study and divided into 4 subgroups according to age at surgery (15 patients in the < 1 month group, 27 in the 1-2 months group, 14 in the 2-3 months group and 17 in the > 3 months group). Eighty-five healthy infants were recruited and divided into 4 age groups (29 in the < 1 month group, 20 in the 1-2 month group, 19 in the 2-3 month group and 17 in the > 3 month group). Preoperative data were collected and compared between CC patients and healthy controls in 4 age groups. Additionally, 73 patients were divided into laparoscopic and open groups to compare postoperative recovery indices and the occurrence of complications to determine the safety and feasibility of laparoscopic CC application in neonates and young infants.
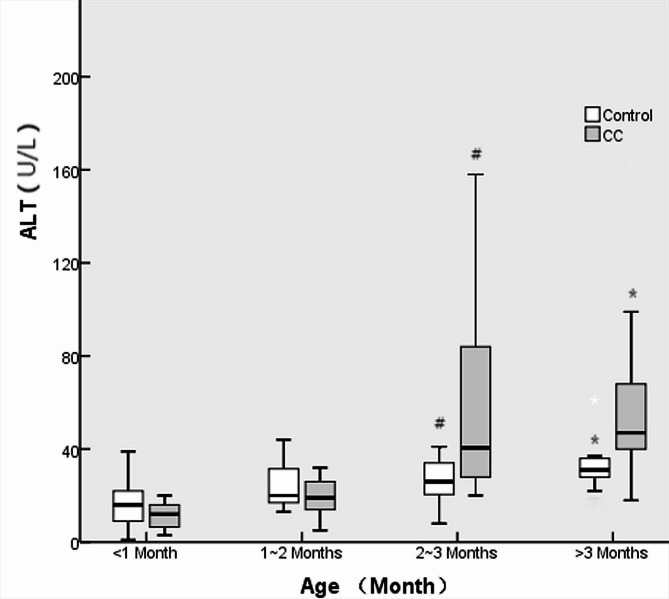
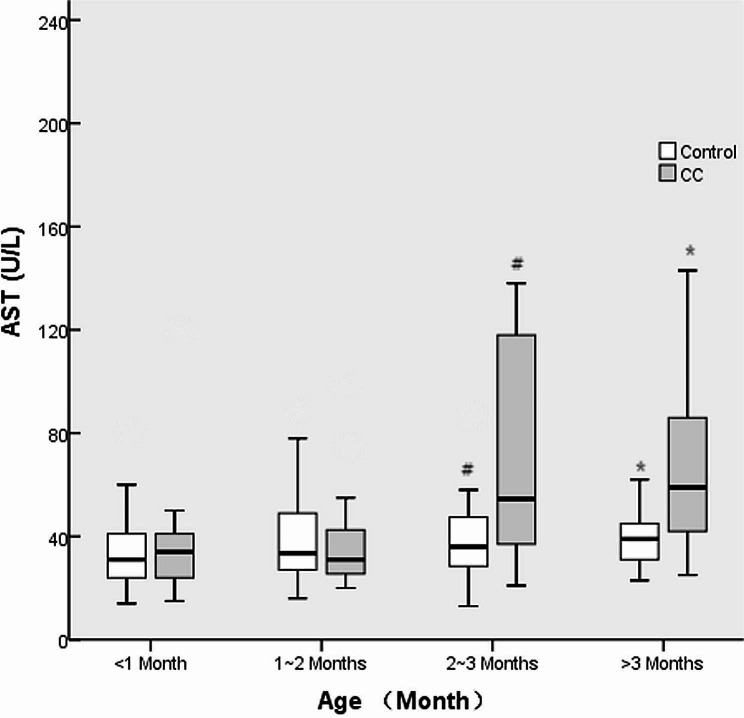
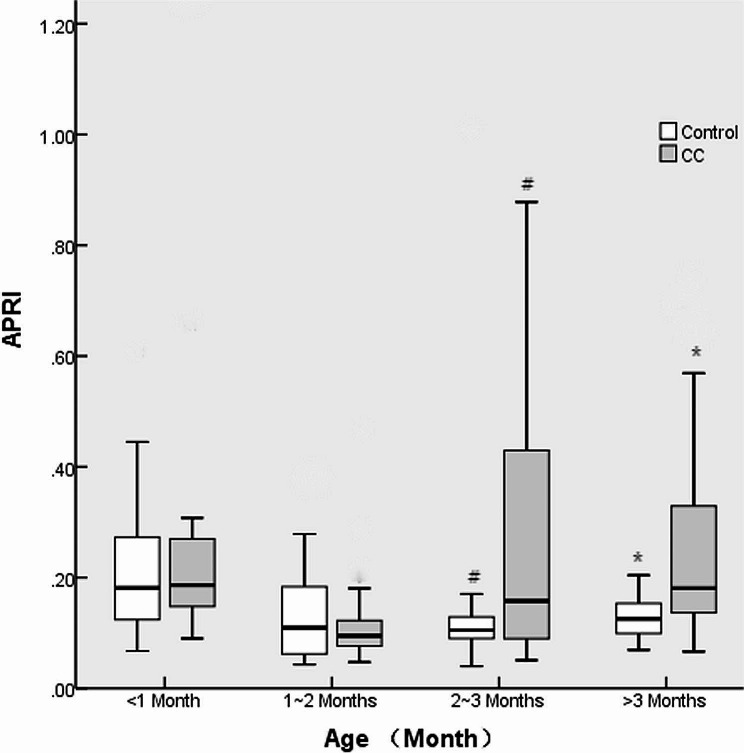
Results: Twenty-one of 73 (28.8%) patients who were prenatally diagnosed with CCs experienced various clinical symptoms, and 15 of 21 (71.4%) patients experienced clinical symptoms less than 2 months after birth. No differences were found in alanine transaminase (ALT), aspartate transaminase (AST) or aspartate transaminase (APRI) levels between CC patients and controls at ≤ 1 month or 1-2 months of age (all p > 0.05), while higher levels were found in CC patients at 2-3 months or > 3 months of age (all p < 0.05). ALT, AST and DBIL levels 1 week after surgery were significantly lower than those before surgery in CC patients who underwent laparoscopic CC excision at > 2 months of age, while DBIL levels 1 week after surgery were also significantly lower than those before surgery in patients who underwent CC excision at ≤ 2 months of age. The initial oral feeding time in the laparoscopic surgery group was significantly earlier than that in the open surgery group for both CC patients who underwent CC excision at ≤ 2 months of age and those > 2 months of age (all p < 0.05). No differences were found in the rates of anastomotic leakage or stricture formation between the laparoscopic and open surgery groups at ≤ 2 months or > 2 months of age.
Conclusion: Most clinical symptoms attributed to CC occur less than 2 months after birth, while liver function and liver fibrosis may deteriorate after 2 months of age in patients with prenatally diagnosed CC. Laparoscopic surgery for CC in newborns and young infants (either less than or more than 2 months old) is safe and feasible and can shorten the initial oral feeding time without increasing complications such as postoperative anastomotic leakage or stricture. Thus, performing laparoscopic CC excisions within 2 months after birth in patients with prenatally diagnosed CC may be appropriate.
Keywords: Choledochal cyst; Minimally invasive; Newborn; Timing of surgery; Young infant.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Timing of surgery for prenatally diagnosed asymptomatic choledochal cysts: a prospective randomized study.J Pediatr Surg. 2012 Mar;47(3):506-12. doi: 10.1016/j.jpedsurg.2011.09.056. J Pediatr Surg. 2012. PMID: 22424346 Clinical Trial.
-
Timing of operation in children with a prenatal diagnosis of choledochal cyst: A single-center retrospective study.J Hepatobiliary Pancreat Sci. 2022 Dec;29(12):1308-1315. doi: 10.1002/jhbp.1155. Epub 2022 May 10. J Hepatobiliary Pancreat Sci. 2022. PMID: 35435313
-
Laparoscopic management for prenatally diagnosed choledochal cysts.Surg Today. 2016 Dec;46(12):1410-1414. doi: 10.1007/s00595-016-1319-3. Epub 2016 Mar 2. Surg Today. 2016. PMID: 26935547
-
Comparison of efficacy and safety of laparoscopic excision and open operation in children with choledochal cysts: A systematic review and update meta-analysis.PLoS One. 2020 Sep 28;15(9):e0239857. doi: 10.1371/journal.pone.0239857. eCollection 2020. PLoS One. 2020. PMID: 32986787 Free PMC article.
-
Choledochal cyst.Pediatr Surg Int. 2023 Jun 1;39(1):209. doi: 10.1007/s00383-023-05483-1. Pediatr Surg Int. 2023. PMID: 37261604 Review.
Cited by
-
Choledochal Cyst and Right Congenital Diaphragmatic Hernia: When to Intervene?European J Pediatr Surg Rep. 2024 Oct 28;12(1):e68-e72. doi: 10.1055/s-0044-1791813. eCollection 2024 Jan. European J Pediatr Surg Rep. 2024. PMID: 39474258 Free PMC article.
-
Laparoscopic Excision of Choledochal Cysts with Roux-en-Y Hepaticojejunostomy in Children: Surgical Technique, Experience, and Outcomes.J Indian Assoc Pediatr Surg. 2025 Jul-Aug;30(4):497-507. doi: 10.4103/jiaps.jiaps_17_25. Epub 2025 Apr 18. J Indian Assoc Pediatr Surg. 2025. PMID: 40756051 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
