

The Second International Consensus Guidelines on the Management of BK Polyomavirus in Kidney Transplantation
- PMID: 38605438
- PMCID: PMC11335089
- DOI: 10.1097/TP.0000000000004976
The Second International Consensus Guidelines on the Management of BK Polyomavirus in Kidney Transplantation
Abstract
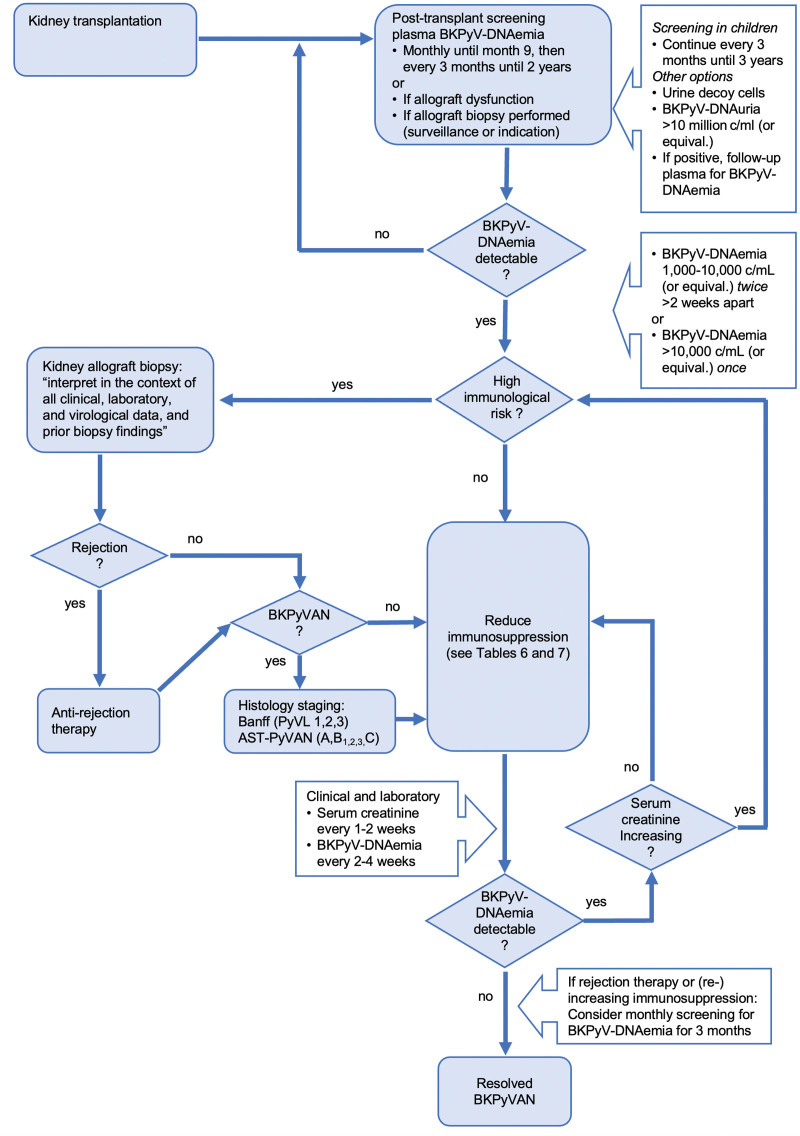
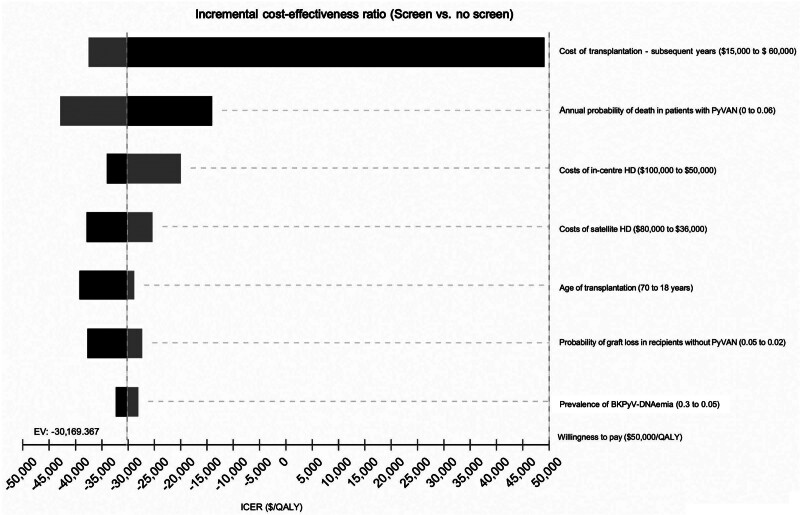
BK polyomavirus (BKPyV) remains a significant challenge after kidney transplantation. International experts reviewed current evidence and updated recommendations according to Grading of Recommendations, Assessment, Development, and Evaluations (GRADE). Risk factors for BKPyV-DNAemia and biopsy-proven BKPyV-nephropathy include recipient older age, male sex, donor BKPyV-viruria, BKPyV-seropositive donor/-seronegative recipient, tacrolimus, acute rejection, and higher steroid exposure. To facilitate early intervention with limited allograft damage, all kidney transplant recipients should be screened monthly for plasma BKPyV-DNAemia loads until month 9, then every 3 mo until 2 y posttransplant (3 y for children). In resource-limited settings, urine cytology screening at similar time points can exclude BKPyV-nephropathy, and testing for plasma BKPyV-DNAemia when decoy cells are detectable. For patients with BKPyV-DNAemia loads persisting >1000 copies/mL, or exceeding 10 000 copies/mL (or equivalent), or with biopsy-proven BKPyV-nephropathy, immunosuppression should be reduced according to predefined steps targeting antiproliferative drugs, calcineurin inhibitors, or both. In adults without graft dysfunction, kidney allograft biopsy is not required unless the immunological risk is high. For children with persisting BKPyV-DNAemia, allograft biopsy may be considered even without graft dysfunction. Allograft biopsies should be interpreted in the context of all clinical and laboratory findings, including plasma BKPyV-DNAemia. Immunohistochemistry is preferred for diagnosing biopsy-proven BKPyV-nephropathy. Routine screening using the proposed strategies is cost-effective, improves clinical outcomes and quality of life. Kidney retransplantation subsequent to BKPyV-nephropathy is feasible in otherwise eligible recipients if BKPyV-DNAemia is undetectable; routine graft nephrectomy is not recommended. Current studies do not support the usage of leflunomide, cidofovir, quinolones, or IVIGs. Patients considered for experimental treatments (antivirals, vaccines, neutralizing antibodies, and adoptive T cells) should be enrolled in clinical trials.
Trial registration: ClinicalTrials.gov NCT05224583.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
C.N.K. received grants from Biohope and funding for serving on scientific advisory boards for Roche Diagnostics. N.K. received consulting fees, honoraria, and travel support from Astellas, AstraZeneca, Biotest, CSL Behring, Chiesi, Gilead, Hansa, Merck, Sharp and Dohme, Glasgow Smith Kline, Neovii, Novartis Pharma, Roche, Sanofi, Sandoz, and Takeda. P.R. received consulting fees from Allovir. M.S. received consulting fees from Merck, Sharp and Dohme, Moderna, and Biotest and honoraria from Biotest, Novartis, Merck, Sharp and Dohme, Takeda, and Qiagen. P.C. received honoraria from Atara Bio and Pierre Fabre Pharma. H.T.S. received grants from Biohope, Merck Sharp and Dohme, Natera, Novartis, and Takeda; honoraria from Alexion, CareDx, EMS Pharmaceuticals, Natera, and Takeda; and consulting fees and travel support from Takeda. D.C.B. received grants from CareDx and VeraTherapeutics and consulting fees from CareDx, Medeor Therapeutics, Natera, Sanofi, and Vera Therapeutics. L.P. received grants from Alexion, Chiesi, and Novartis; consulting fees from Alnylam and Chiesi; and travel support from Alexion. H.H.H. received consulting fees from AICuris, Allovir, Moderna, VeraTX, and Roche and honoraria from VeraTX, Takeda, Biotest, and Gilead. The other authors declare no conflicts of interest.
Figures
Comment in
-
Comments on: The Second International Consensus Guidelines on the Management of BK Polyomavirus in Kidney Transplantation.Transplantation. 2024 Sep 1;108(9):e276. doi: 10.1097/TP.0000000000005087. Epub 2024 Aug 21. Transplantation. 2024. PMID: 39166903 Free PMC article. No abstract available.
References
-
- Wu Z, Graf FE, Hirsch HH. Antivirals against human polyomaviruses: leaving no stone unturned. Rev Med Virol. 2021;31:e2220. - PubMed
-
- Hirsch HH, Brennan DC, Drachenberg CB, et al. Polyomavirus-associated nephropathy in renal transplantation: interdisciplinary analyses and recommendations. Transplantation. 2005;79:1277–1286. - PubMed
-
- Kotton CN, Kumar D, Caliendo AM, et al. ; The Transplantation Society International CMV Consensus Group. The third international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2018;102:900–931. - PubMed
-
- Hirsch HH, Randhawa PS; AST Infectious Diseases Community of Practice. BK polyomavirus in solid organ transplantation—guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33:e13528. - PubMed
-
- Leuzinger K, Naegele K, Schaub S, et al. Quantification of plasma BK polyomavirus loads is affected by sequence variability, amplicon length, and non-encapsidated viral DNA genome fragments. J Clin Virol. 2019;121:104210. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
