

Anticoagulation for Patients With Concomitant Atrial Fibrillation and End-Stage Renal Disease: A Systematic Review and Network Meta-Analysis
- PMID: 38606775
- PMCID: PMC11262503
- DOI: 10.1161/JAHA.123.034176
Anticoagulation for Patients With Concomitant Atrial Fibrillation and End-Stage Renal Disease: A Systematic Review and Network Meta-Analysis
Abstract
Background: Concomitant atrial fibrillation and end-stage renal disease is common and associated with an unfavorable prognosis. Although oral anticoagulants have been well established to prevent thromboembolism, the applicability in patients under long-term dialysis remains debatable. The study aimed to determine the efficacy and safety of anticoagulation in the dialysis-dependent population.
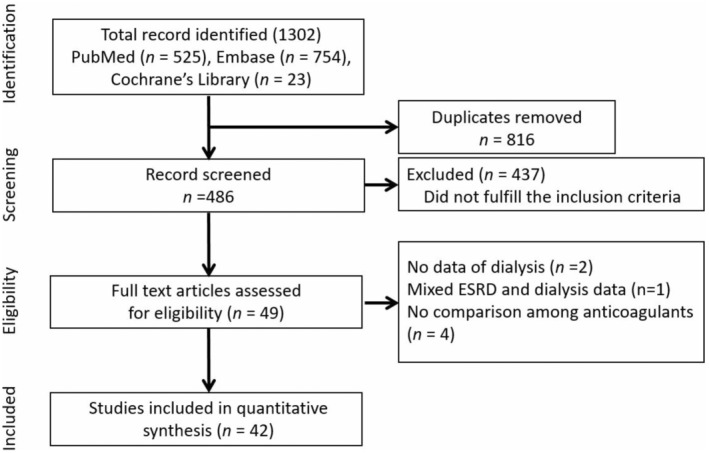
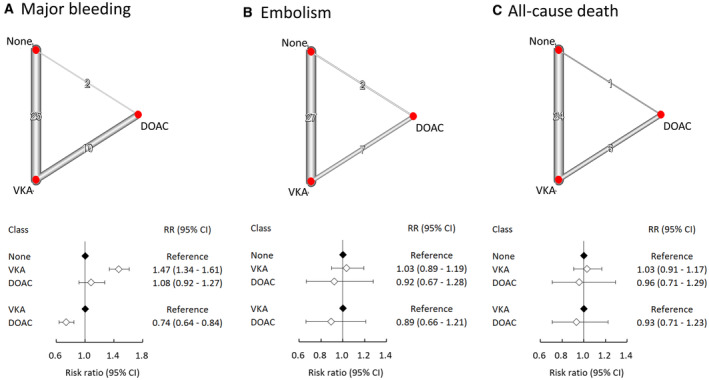
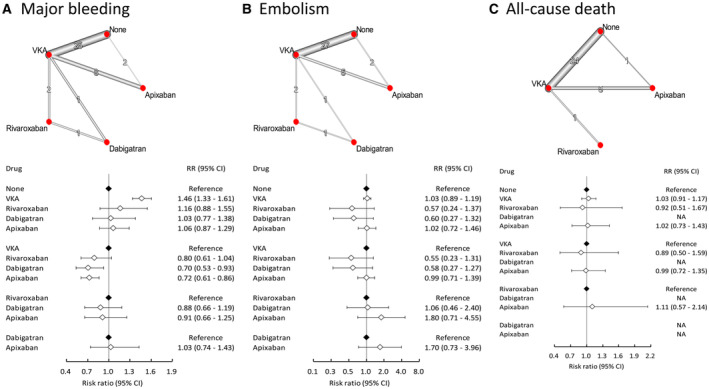
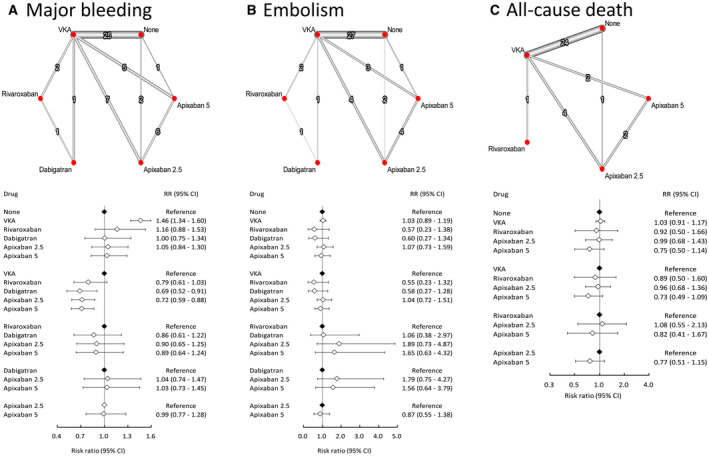
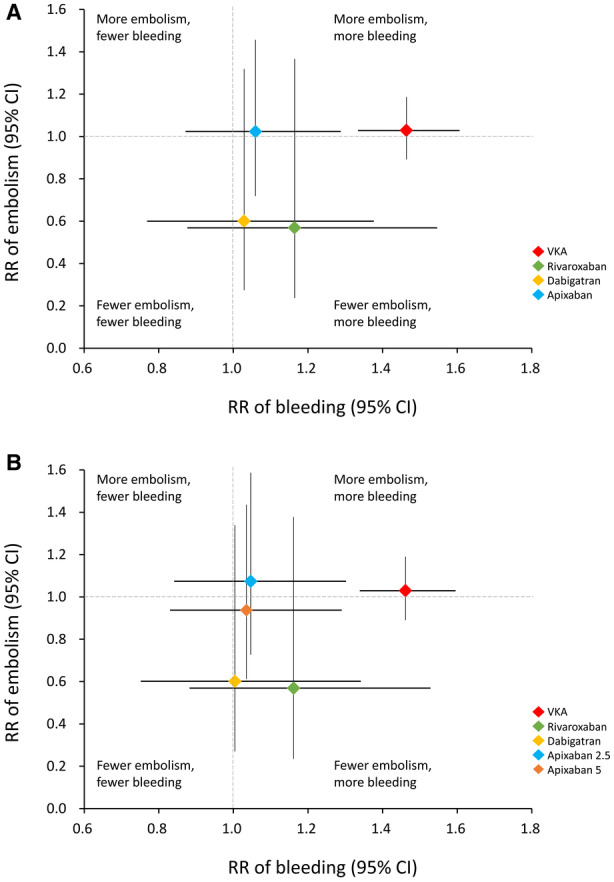
Methods and results: An updated network meta-analysis based on MEDLINE, EMBASE, and the Cochrane Library was performed. Studies published up to December 2022 were included. Direct oral anticoagulants (DOACs, dabigatran, rivaroxaban, apixaban 2.5/5 mg twice daily), vitamin K antagonists (VKAs), and no anticoagulation were compared on safety and efficacy outcomes. The outcomes of interest were major bleeding, thromboembolism, and all-cause death. A total of 42 studies, including 3 randomized controlled trials, with 185 864 subjects were pooled. VKAs were associated with a significantly higher risk of major bleeding than either no anticoagulation (hazard ratio [HR], 1.47; 95% CI, 1.34-1.61) or DOACs (DOACs versus VKAs; HR, 0.74 [95% CI, 0.64-0.84]). For the prevention of thromboembolism, the efficacies of VKAs, DOACs, and no anticoagulation were equivalent. Nevertheless, dabigatran and rivaroxaban were associated with fewer embolic events. There were no differences in all-cause death with the administration of VKAs, DOACs, or no anticoagulation.
Conclusions: For dialysis-dependent populations, dabigatran and rivaroxaban were associated with better efficacy, while dabigatran and apixaban demonstrated better safety. No anticoagulation was a noninferior alterative, and VKAs were associated with the worst outcomes.
Keywords: anticoagulation; atrial fibrillation; chronic kidney disease; dialysis; meta‐analysis.
Figures
Similar articles
-
An Evidence-Based Approach to Anticoagulation Therapy Comparing Direct Oral Anticoagulants and Vitamin K Antagonists in Patients With Atrial Fibrillation and Bioprosthetic Valves: A Systematic Review, Meta-Analysis, and Network Meta-Analysis.Am J Cardiol. 2023 Nov 1;206:132-150. doi: 10.1016/j.amjcard.2023.07.141. Epub 2023 Sep 11. Am J Cardiol. 2023. PMID: 37703679
-
Effectiveness and Safety of Non-vitamin K Antagonist Oral Anticoagulants for Atrial Fibrillation and Venous Thromboembolism: A Systematic Review and Meta-analyses.Clin Ther. 2017 Jul;39(7):1456-1478.e36. doi: 10.1016/j.clinthera.2017.05.358. Epub 2017 Jun 28. Clin Ther. 2017. PMID: 28668628
-
Anticoagulation for the long-term treatment of venous thromboembolism in people with cancer.Cochrane Database Syst Rev. 2018 Jun 19;6(6):CD006650. doi: 10.1002/14651858.CD006650.pub5. Cochrane Database Syst Rev. 2018. PMID: 29920657 Free PMC article.
-
Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis.BMJ. 2017 Nov 28;359:j5058. doi: 10.1136/bmj.j5058. BMJ. 2017. PMID: 29183961 Free PMC article.
-
Left Atrial Appendage Closure Compared With Oral Anticoagulants for Patients With Atrial Fibrillation: A Systematic Review and Network Meta-Analysis.J Am Heart Assoc. 2024 Aug 20;13(16):e034815. doi: 10.1161/JAHA.124.034815. Epub 2024 Aug 9. J Am Heart Assoc. 2024. PMID: 39119987 Free PMC article.
Cited by
-
Treatment strategies of the thromboembolic risk in kidney failure patients with atrial fibrillation.Nephrol Dial Transplant. 2024 Jul 31;39(8):1248-1257. doi: 10.1093/ndt/gfae121. Nephrol Dial Transplant. 2024. PMID: 38816212 Free PMC article. Review.
-
Pulmonary Embolism in Patients with End-Stage Kidney Disease Starting Dialysis.JAMA Netw Open. 2025 Mar 3;8(3):e250848. doi: 10.1001/jamanetworkopen.2025.0848. JAMA Netw Open. 2025. PMID: 40094668 Free PMC article.
-
Atrial Fibrillation Is Associated With Increased In-Hospital and 1-Year Mortality in Patients Receiving Hemodialysis With ST Elevation Myocardial Infarction: A Retrospective Cohort Study.Kidney Med. 2025 May 12;7(7):101023. doi: 10.1016/j.xkme.2025.101023. eCollection 2025 Jul. Kidney Med. 2025. PMID: 40613014 Free PMC article.
-
Anticoagulation Strategies for Atrial Fibrillation in CKD Stage G5 and Dialysis Patients: An Updated Scoping Review.Rev Cardiovasc Med. 2025 Mar 5;26(3):26736. doi: 10.31083/RCM26736. eCollection 2025 Mar. Rev Cardiovasc Med. 2025. PMID: 40160594 Free PMC article. Review.
-
Hallmarks for Thrombotic and Hemorrhagic Risks in Chronic Kidney Disease Patients.Int J Mol Sci. 2024 Aug 9;25(16):8705. doi: 10.3390/ijms25168705. Int J Mol Sci. 2024. PMID: 39201390 Free PMC article. Review.
References
-
- Genovesi S, Pogliani D, Faini A, Valsecchi MG, Riva A, Stefani F, Acquistapace I, Stella A, Bonforte G, DeVecchi A, et al. Prevalence of atrial fibrillation and associated factors in a population of long‐term hemodialysis patients. Am J Kidney Dis. 2005;46:897–902. doi: 10.1053/j.ajkd.2005.07.044 - DOI - PubMed
-
- Soliman EZ, Prineas RJ, Go AS, Xie D, Lash JP, Rahman M, Ojo A, Teal VL, Jensvold NG, Robinson NL, et al. Chronic renal insufficiency cohort (CRIC) study group. Chronic kidney disease and prevalent atrial fibrillation: the chronic renal insufficiency cohort (CRIC). Am Heart J. 2010;159:1102–1107. doi: 10.1016/j.ahj.2010.03.027 - DOI - PMC - PubMed
-
- Randhawa MS, Vishwanath R, Rai MP, Wang L, Randhawa AK, Abela G, Dhar G. Association between use of warfarin for atrial fibrillation and outcomes among patients with end stage renal disease: a systematic review and meta‐analysis. JAMA Netw Open. 2020;3:e202175. doi: 10.1001/jamanetworkopen.2020.2175 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
