

Atherosclerosis evaluation and cardiovascular risk estimation using coronary computed tomography angiography
- PMID: 38606889
- PMCID: PMC11129796
- DOI: 10.1093/eurheartj/ehae190
Atherosclerosis evaluation and cardiovascular risk estimation using coronary computed tomography angiography
Erratum in
-
Correction to: Atherosclerosis evaluation and cardiovascular risk estimation using coronary computed tomography angiography.Eur Heart J. 2024 Jul 9;45(26):2332. doi: 10.1093/eurheartj/ehae318. Eur Heart J. 2024. PMID: 38748452 Free PMC article. No abstract available.
Abstract
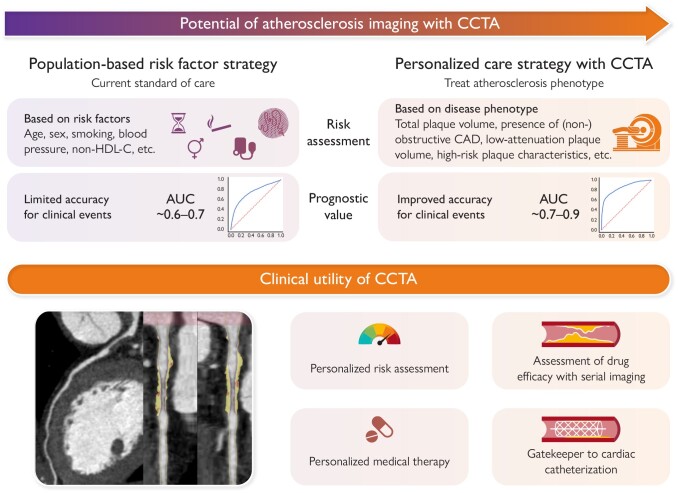
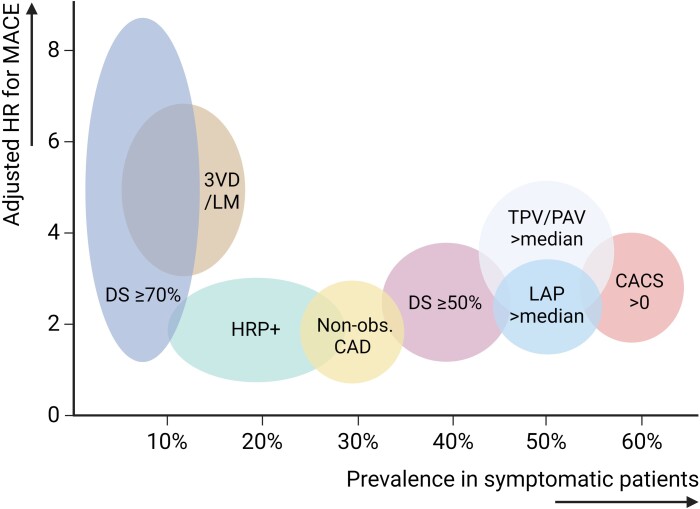
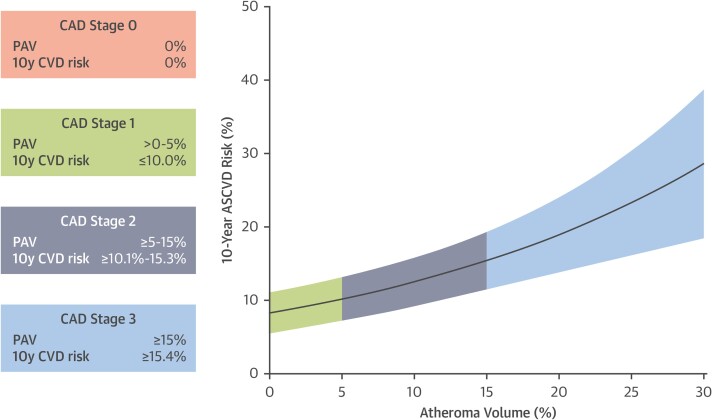
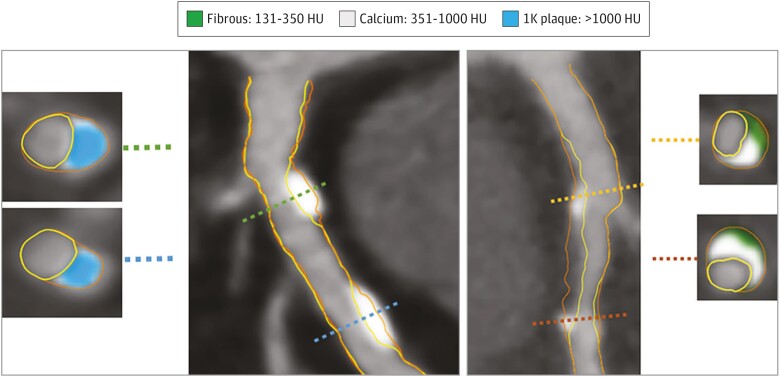
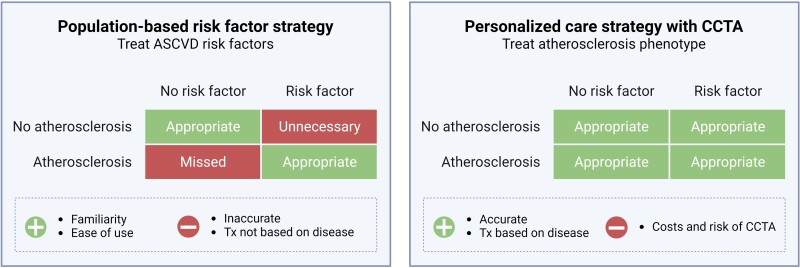
Clinical risk scores based on traditional risk factors of atherosclerosis correlate imprecisely to an individual's complex pathophysiological predisposition to atherosclerosis and provide limited accuracy for predicting major adverse cardiovascular events (MACE). Over the past two decades, computed tomography scanners and techniques for coronary computed tomography angiography (CCTA) analysis have substantially improved, enabling more precise atherosclerotic plaque quantification and characterization. The accuracy of CCTA for quantifying stenosis and atherosclerosis has been validated in numerous multicentre studies and has shown consistent incremental prognostic value for MACE over the clinical risk spectrum in different populations. Serial CCTA studies have advanced our understanding of vascular biology and atherosclerotic disease progression. The direct disease visualization of CCTA has the potential to be used synergistically with indirect markers of risk to significantly improve prevention of MACE, pending large-scale randomized evaluation.
Keywords: Atherosclerotic cardiovascular disease; Coronary artery disease; Coronary computed tomography angiography; Major adverse cardiovascular events; Prevention.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019;140:e596–646. 10.1161/CIR.0000000000000678 - DOI - PMC - PubMed
