

Maternal tadalafil treatment does not increase uterine artery blood flow or oxygen delivery in the pregnant ewe
- PMID: 38606906
- PMCID: PMC11140180
- DOI: 10.1113/EP091593
Maternal tadalafil treatment does not increase uterine artery blood flow or oxygen delivery in the pregnant ewe
Abstract
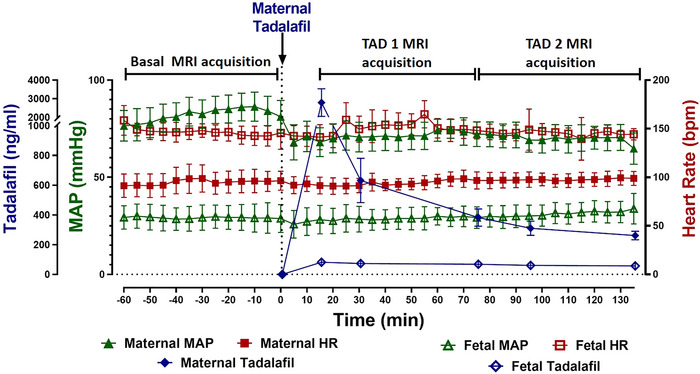
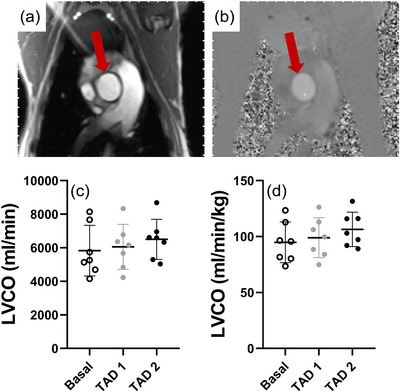
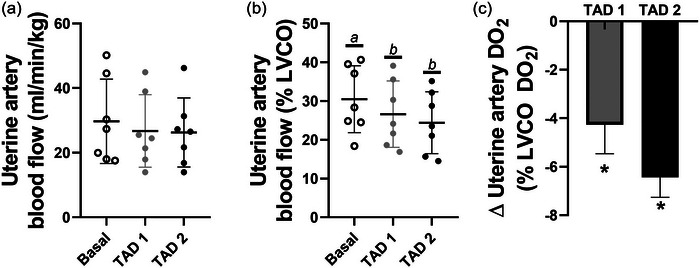
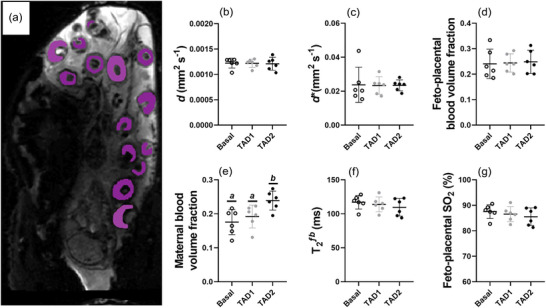
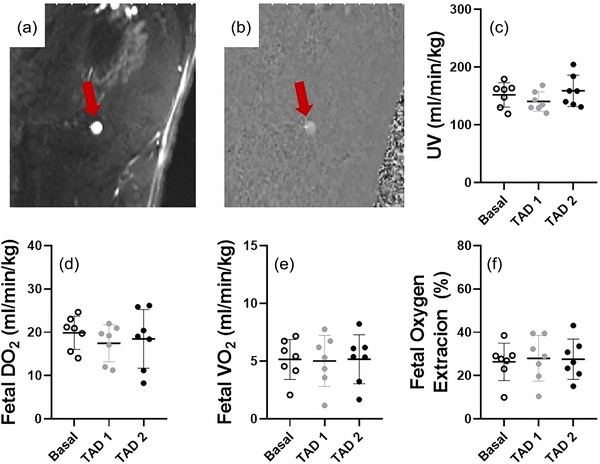
Increasing placental perfusion (PP) could improve outcomes of growth-restricted fetuses. One way of increasing PP may be by using phosphodiesterase (PDE)-5 inhibitors, which induce vasodilatation of vascular beds. We used a combination of clinically relevant magnetic resonance imaging (MRI) techniques to characterize the impact that tadalafil infusion has on maternal, placental and fetal circulations. At 116-117 days' gestational age (dGA; term, 150 days), pregnant ewes (n = 6) underwent fetal catheterization surgery. At 120-123 dGA ewes were anaesthetized and MRI scans were performed during three acquisition windows: a basal state and then ∼15-75 min (TAD 1) and ∼75-135 min (TAD 2) post maternal administration (24 mg; intravenous bolus) of tadalafil. Phase contrast MRI and T2 oximetry were used to measure blood flow and oxygen delivery. Placental diffusion and PP were assessed using the Diffusion-Relaxation Combined Imaging for Detailed Placental Evaluation-'DECIDE' technique. Uterine artery (UtA) blood flow when normalized to maternal left ventricular cardiac output (LVCO) was reduced in both TAD periods. DECIDE imaging found no impact of tadalafil on placental diffusivity or fetoplacental blood volume fraction. Maternal-placental blood volume fraction was increased in the TAD 2 period. Fetal and were not affected by maternal tadalafil administration. Maternal tadalafil administration did not increase UtA blood flow and thus may not be an effective vasodilator at the level of the UtAs. The increased maternal-placental blood volume fraction may indicate local vasodilatation of the maternal intervillous space, which may have compensated for the reduced proportion of UtA .
Keywords: fetal MRI; fetal development; fetal growth restriction; haemodynamics; magnetic resonance imaging; placental perfusion; tadafer; tadalafil.
© 2024 The Authors. Experimental Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
An MRI approach to assess placental function in healthy humans and sheep.J Physiol. 2021 May;599(10):2573-2602. doi: 10.1113/JP281002. Epub 2021 Mar 29. J Physiol. 2021. PMID: 33675040
-
Impact of resveratrol-mediated increase in uterine artery blood flow on fetal haemodynamics, blood pressure and oxygenation in sheep.Exp Physiol. 2021 May;106(5):1166-1180. doi: 10.1113/EP089237. Epub 2021 Mar 16. Exp Physiol. 2021. PMID: 33600040
-
Feasibility of multimodal magnetic resonance imaging to assess maternal hyperoxygenation in sheep pregnancy.J Physiol. 2025 Mar;603(5):1029-1044. doi: 10.1113/JP287272. Epub 2025 Feb 12. J Physiol. 2025. PMID: 39937834 Free PMC article.
-
Pathophysiology of placental-derived fetal growth restriction.Am J Obstet Gynecol. 2018 Feb;218(2S):S745-S761. doi: 10.1016/j.ajog.2017.11.577. Am J Obstet Gynecol. 2018. PMID: 29422210 Review.
-
Humans at high altitude: hypoxia and fetal growth.Respir Physiol Neurobiol. 2011 Aug 31;178(1):181-90. doi: 10.1016/j.resp.2011.04.017. Epub 2011 Apr 22. Respir Physiol Neurobiol. 2011. PMID: 21536153 Free PMC article. Review.
Cited by
-
Advanced magnetic resonance imaging in human placenta: insights into fetal growth restriction and congenital heart disease.Front Cardiovasc Med. 2024 Jul 23;11:1426593. doi: 10.3389/fcvm.2024.1426593. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39108671 Free PMC article. Review.
-
Maternal obesogenic diet during pregnancy and its impact on fetal hepatic function in baboons.Obesity (Silver Spring). 2024 Oct;32(10):1910-1922. doi: 10.1002/oby.24124. Epub 2024 Aug 29. Obesity (Silver Spring). 2024. PMID: 39210592
References
-
- Aughwane, R. , Mufti, N. , Flouri, D. , Maksym, K. , Spencer, R. , Sokolska, M. , Kendall, G. , Atkinson, D. , Bainbridge, A. , Deprest, J. , Vercauteren, T. , Ourselin, S. , David, A. L. , & Melbourne, A. (2021). Magnetic resonance imaging measurement of placental perfusion and oxygen saturation in early‐onset fetal growth restriction. British Journal of Obstetrics and Gynaecology, 128(2), 337–345. - PMC - PubMed
-
- Bukowski, R. , Hansen, N. I. , Willinger, M. , Reddy, U. M. , Parker, C. B. , Pinar, H. , Silver, R. M. , Dudley, D. J. , Stoll, B. J. , Saade, G. R. , Koch, M. A. , Rowland Hogue, C. J. , Varner, M. W. , Conway, D. L. , Coustan, D. , & Goldenberg, R. L , Eunice Kennedy Shriver National Institute of Child H & Human Development Stillbirth Collaborative Research N . (2014). Fetal growth and risk of stillbirth: A population‐based case‐control study. PLoS Medicine, 11(4), e1001633. - PMC - PubMed
-
- Cho, S. K. S. , Darby, J. R. T. , Saini, B. S. , Lock, M. C. , Holman, S. L. , Lim, J. M. , Perumal, S. R. , Macgowan, C. K. , Morrison, J. L. , & Seed, M. (2020). Feasibility of ventricular volumetry by cardiovascular MRI to assess cardiac function in the fetal sheep. The Journal of Physiology, 598(13), 2557–2573. - PubMed
-
- Darby, J. R. T. (2020). Sildenafil: How to make a bad situation worse. The Journal of Physiology, 598(19), 4139–4140. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous