

Satellite Glial Cells in Human Disease
- PMID: 38607005
- PMCID: PMC11011452
- DOI: 10.3390/cells13070566
Satellite Glial Cells in Human Disease
Abstract
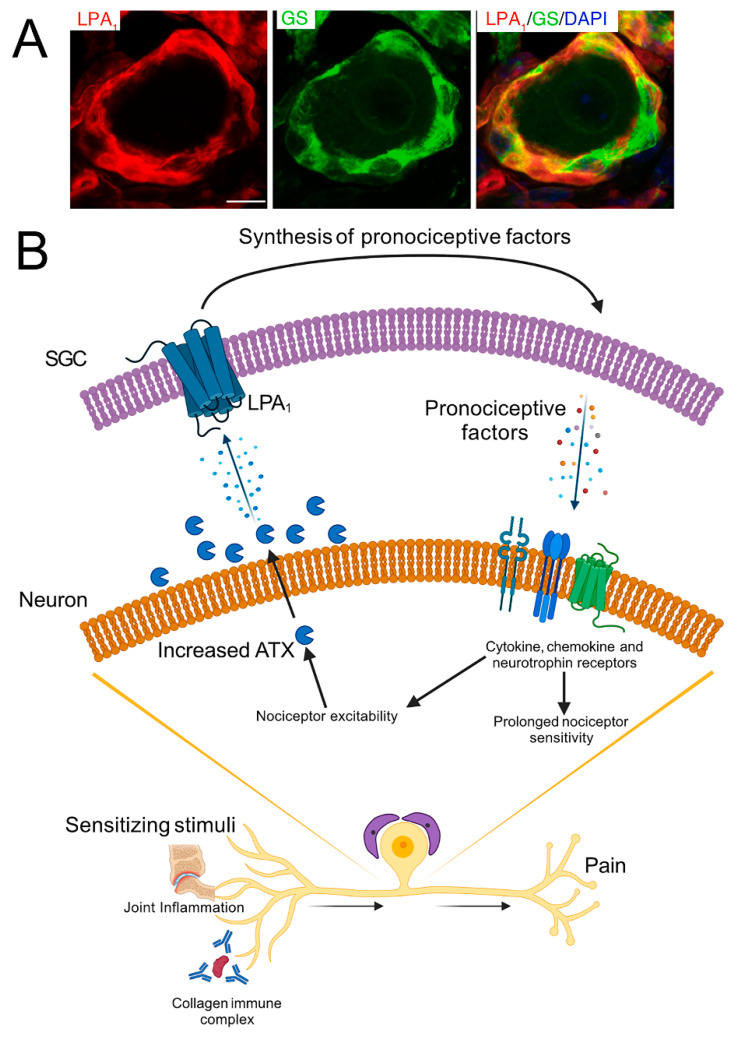
Satellite glial cells (SGCs) are the main type of glial cells in sensory ganglia. Animal studies have shown that these cells play essential roles in both normal and disease states. In a large number of pain models, SGCs were activated and contributed to the pain behavior. Much less is known about SGCs in humans, but there is emerging recognition that SGCs in humans are altered in a variety of clinical states. The available data show that human SGCs share some essential features with SGCs in rodents, but many differences do exist. SGCs in DRG from patients suffering from common painful diseases, such as rheumatoid arthritis and fibromyalgia, may contribute to the pain phenotype. It was found that immunoglobulins G (IgG) from fibromyalgia patients can induce pain-like behavior in mice. Moreover, these IgGs bind preferentially to SGCs and activate them, which can sensitize the sensory neurons, causing nociception. In other human diseases, the evidence is not as direct as in fibromyalgia, but it has been found that an antibody from a patient with rheumatoid arthritis binds to mouse SGCs, which leads to the release of pronociceptive factors from them. Herpes zoster is another painful disease, and it appears that the zoster virus resides in SGCs, which acquire an abnormal morphology and may participate in the infection and pain generation. More work needs to be undertaken on SGCs in humans, and this review points to several promising avenues for better understanding disease mechanisms and developing effective pain therapies.
Keywords: autoimmune diseases; dorsal root ganglion; fibromyalgia; herpes; rheumatoid arthritis; satellite glial cells; sensory neuron; trigeminal ganglion.
Conflict of interest statement
The author declares no conflicts of interest.
Figures
Similar articles
-
Satellite glial cell-secreted exosomes after in-vitro oxaliplatin treatment presents a pro-nociceptive effect for dorsal root ganglion neurons and induce mechanical hypersensitivity in naïve mice.Mol Cell Neurosci. 2023 Sep;126:103881. doi: 10.1016/j.mcn.2023.103881. Epub 2023 Jul 18. Mol Cell Neurosci. 2023. PMID: 37467904
-
Satellite Glial Cells Give Rise to Nociceptive Sensory Neurons.Stem Cell Rev Rep. 2021 Jun;17(3):999-1013. doi: 10.1007/s12015-020-10102-w. Epub 2021 Jan 3. Stem Cell Rev Rep. 2021. PMID: 33389681
-
Bidirectional calcium signaling between satellite glial cells and neurons in cultured mouse trigeminal ganglia.Neuron Glia Biol. 2010 Feb;6(1):43-51. doi: 10.1017/S1740925X09990408. Epub 2009 Nov 6. Neuron Glia Biol. 2010. PMID: 19891813 Free PMC article.
-
Satellite glial cells in sympathetic and parasympathetic ganglia: in search of function.Brain Res Rev. 2010 Sep 24;64(2):304-27. doi: 10.1016/j.brainresrev.2010.04.009. Epub 2010 May 2. Brain Res Rev. 2010. PMID: 20441777 Review.
-
The role of satellite glial cells in orofacial pain.J Neurosci Res. 2019 Apr;97(4):393-401. doi: 10.1002/jnr.24341. Epub 2018 Nov 19. J Neurosci Res. 2019. PMID: 30450738 Review.
Cited by
-
From Gut Motility to Chronic Pain: Studies on the Mammalian Peripheral Nervous System.Bioelectricity. 2024 Sep 16;6(3):207-220. doi: 10.1089/bioe.2024.0036. eCollection 2024 Sep. Bioelectricity. 2024. PMID: 39372092 No abstract available.
-
Schwann Cells in Neuromuscular Disorders: A Spotlight on Amyotrophic Lateral Sclerosis.Cells. 2025 Jan 3;14(1):47. doi: 10.3390/cells14010047. Cells. 2025. PMID: 39791748 Free PMC article. Review.
-
How Do Peripheral Neurons and Glial Cells Participate in Pain Alleviation by Physical Activity?Cells. 2025 Mar 20;14(6):462. doi: 10.3390/cells14060462. Cells. 2025. PMID: 40136711 Free PMC article. Review.
-
Nageotte nodules in human dorsal root ganglia reveal neurodegeneration in diabetic peripheral neuropathy.Nat Commun. 2025 May 5;16(1):4168. doi: 10.1038/s41467-025-59538-z. Nat Commun. 2025. PMID: 40325011 Free PMC article.
-
Pathogenic Crosstalk Between the Peripheral and Central Nervous System in Rheumatic Diseases: Emerging Evidence and Clinical Implications.Int J Mol Sci. 2025 Jun 24;26(13):6036. doi: 10.3390/ijms26136036. Int J Mol Sci. 2025. PMID: 40649815 Free PMC article. Review.
References
-
- Pannese E. Biology and Pathology of Perineuronal Satellite Cells in Sensory Ganglia. Springer; Cham, Switzerland: 2018. pp. 1–83.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
