

Genetic Signature of Human Pancreatic Cancer and Personalized Targeting
- PMID: 38607041
- PMCID: PMC11011857
- DOI: 10.3390/cells13070602
Genetic Signature of Human Pancreatic Cancer and Personalized Targeting
Abstract
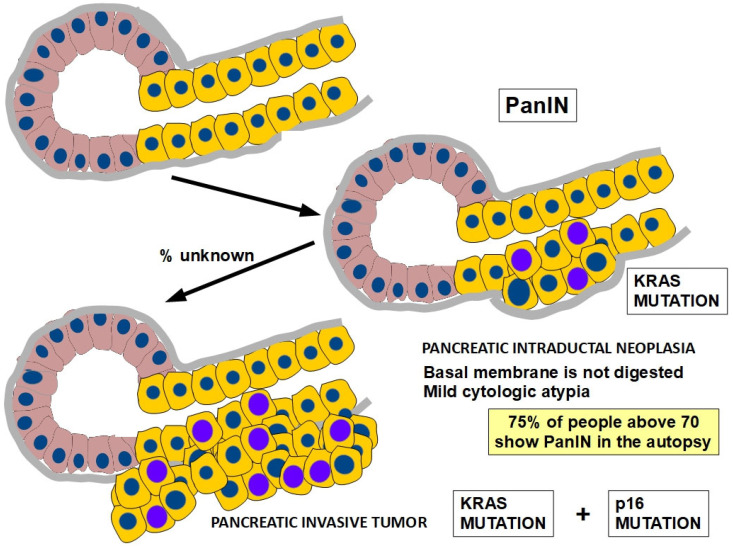
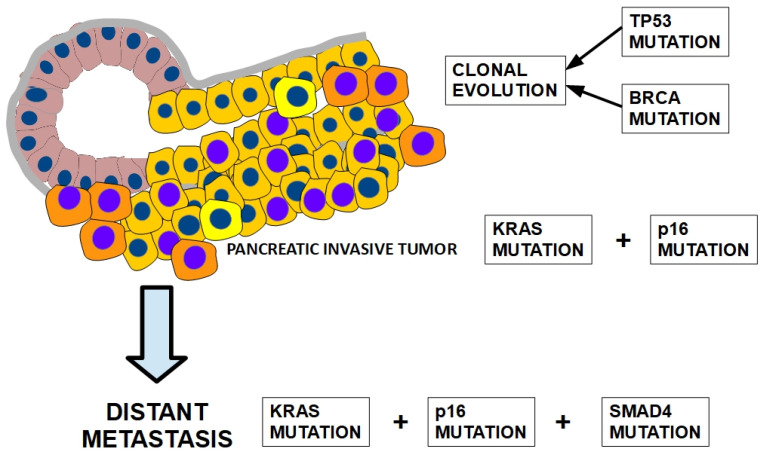
Pancreatic cancer is a highly lethal disease with a 5-year survival rate of around 11-12%. Surgery, being the treatment of choice, is only possible in 20% of symptomatic patients. The main reason is that when it becomes symptomatic, IT IS the tumor is usually locally advanced and/or has metastasized to distant organs; thus, early diagnosis is infrequent. The lack of specific early symptoms is an important cause of late diagnosis. Unfortunately, diagnostic tumor markers become positive at a late stage, and there is a lack of early-stage markers. Surgical and non-surgical cases are treated with neoadjuvant and/or adjuvant chemotherapy, and the results are usually poor. However, personalized targeted therapy directed against tumor drivers may improve this situation. Until recently, many pancreatic tumor driver genes/proteins were considered untargetable. Chemical and physical characteristics of mutated KRAS are a formidable challenge to overcome. This situation is slowly changing. For the first time, there are candidate drugs that can target the main driver gene of pancreatic cancer: KRAS. Indeed, KRAS inhibition has been clinically achieved in lung cancer and, at the pre-clinical level, in pancreatic cancer as well. This will probably change the very poor outlook for this disease. This paper reviews the genetic characteristics of sporadic and hereditary predisposition to pancreatic cancer and the possibilities of a personalized treatment according to the genetic signature.
Keywords: KRAS; PDAC (pancreatic ductal adenocarcinoma); driver mutations; personalized treatment.
Conflict of interest statement
The authors declare no conflicts of interest nor any potential commercial interests.
Figures
References
-
- Subbiah V., Puzanov I., Blay J.-Y., Chau I., Lockhart A.C., Raje N.S., Wolf J., Baselga J., Meric-Bernstam F., Roszik J., et al. Pan-Cancer Efficacy of Vemurafenib in BRAFV600-Mutant Non-Melanoma Cancers. Cancer Discov. 2020;10:657–663. doi: 10.1158/2159-8290.CD-19-1265. - DOI - PMC - PubMed
-
- Kong B., Thoma E., Michalski C.W. From Tissue Turnover to the Cell of Origin of Pancreatic Cancer. In: Beger H.G., Büchler M.W., Hruban R.H., Mayerle J., Neoptolemos J.P., Shimosegawa T., Warshaw A.L., Whitcomb D.C., Zhao Y., Groß C., editors. The Pancreas. Publisher Wiley; Hoboken, NJ, USA: 2023. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
