

Long-term prognostic value of the H2FPEF score in patients undergoing transcatheter aortic valve implantation
- PMID: 38607328
- PMCID: PMC11287290
- DOI: 10.1002/ehf2.14773
Long-term prognostic value of the H2FPEF score in patients undergoing transcatheter aortic valve implantation
Abstract
Aims: A considerable proportion of candidates for transcatheter aortic valve implantation (TAVI) have underlying heart failure (HF) with preserved ejection fraction (HFpEF), which can be challenging for diagnosis because significant valvular heart disease should be excluded before diagnosing HFpEF. This study investigated the long-term prognostic value of the pre-procedural H2FPEF score in patients with preserved ejection fraction (EF) undergoing TAVI.
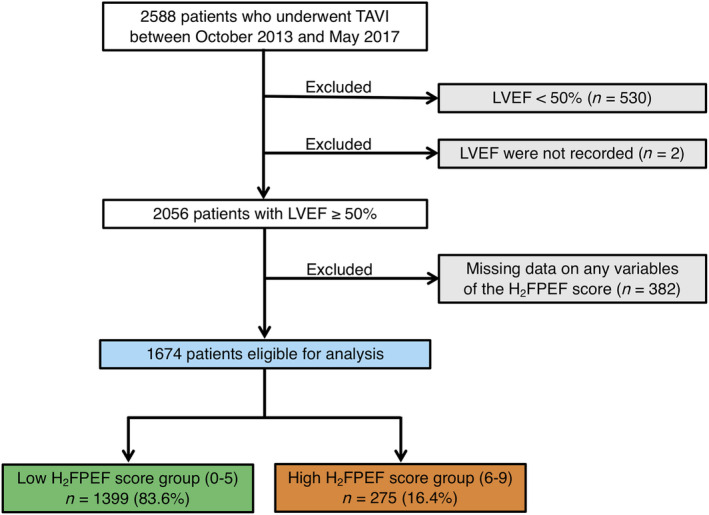
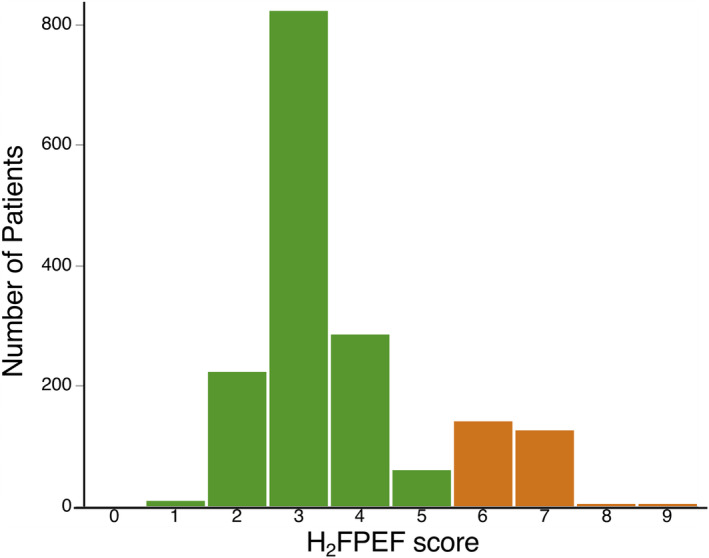
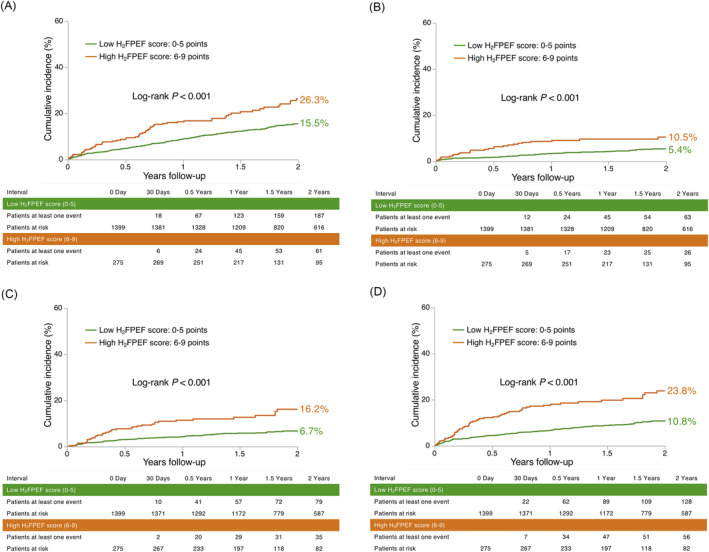
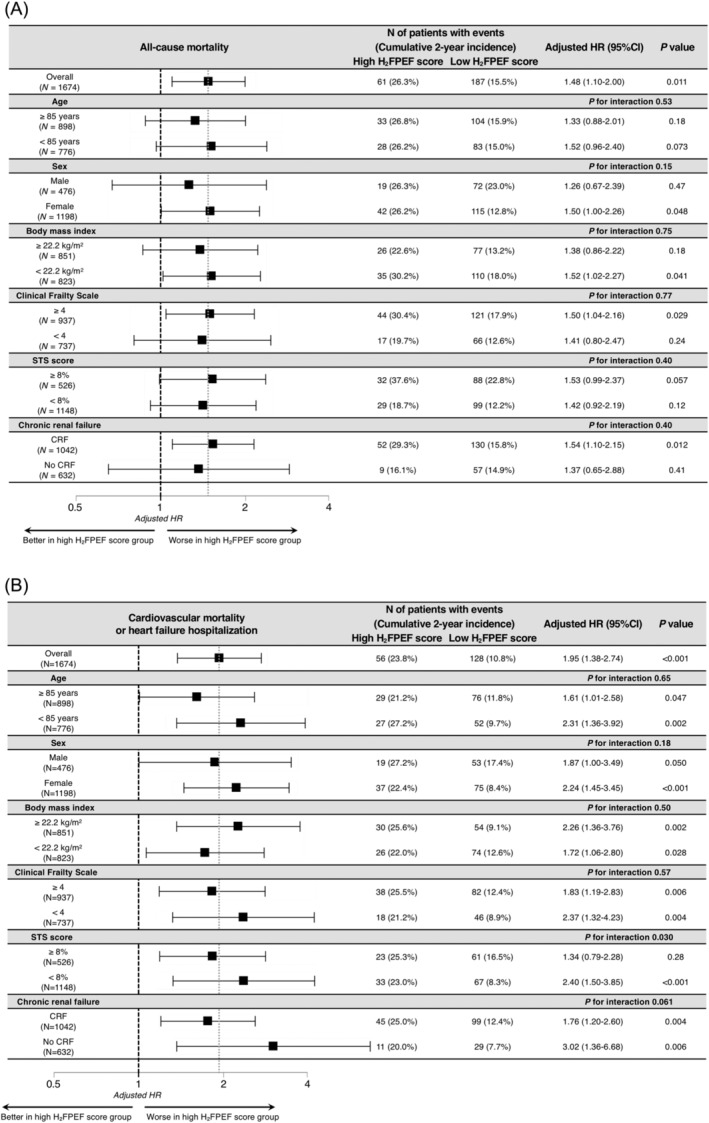
Methods and results: Patients who underwent TAVI between October 2013 and May 2017 were enrolled from the Optimized CathEter vAlvular iNtervention-Transcatheter Aortic Valve Implantation Japanese multicentre registry. After excluding 914 patients, 1674 patients with preserved EF ≥ 50% (median age: 85 years, 72% female) were selected for calculation of the H2FPEF score and were dichotomized into two groups: the low H2FPEF score [0-5 points; n = 1399 (83.6%)] group and the high H2FPEF score [6-9 points; n = 275 (16.4%)] group. Patients with high H2FPEF scores were associated with a higher prevalence of New York Heart Association Functional Class III/IV (59.3% vs. 43.7%, P < 0.001), diabetes (24.4% vs. 18.5%, P = 0.03), and paradoxical low-flow, low-gradient aortic stenosis (15.9% vs. 6.2%, P < 0.001). These patients showed worse prognoses than those with low H2FPEF scores regarding the cumulative 2 year all-cause mortality (26.3% vs. 15.5%, log-rank P < 0.001), cardiovascular mortality (10.5% vs. 5.4%, log-rank P < 0.001), HF hospitalization (16.2% vs. 6.7%, log-rank P < 0.001), and the composite endpoint of cardiovascular mortality and HF hospitalization (23.8% vs. 10.8%, log-rank P < 0.001). After adjustment for several confounders, the high H2FPEF scores were independently associated with increased risk for all-cause mortality [adjusted hazard ratio (HR), 1.48; 95% confidence interval (CI), 1.09-2.00; P = 0.011] and for the composite endpoint of cardiovascular mortality and HF hospitalization (adjusted HR, 1.95; 95% CI, 1.38-2.74; P < 0.001). Subgroup analysis confirmed the excess risk of high H2FPEF scores relative to low H2FPEF scores for the composite endpoint of cardiovascular mortality and HF hospitalization increased with a lower Society of Thoracic Surgeons (STS) score (STS score <8%: adjusted HR, 2.40; 95% CI, 1.50-3.85; P < 0.001; STS score ≥8%: adjusted HR, 1.34; 95% CI, 0.79-2.28; P = 0.28; Pinteraction = 0.030).
Conclusions: The H2FPEF score is useful for predicting long-term adverse outcomes after TAVI, including all-cause mortality, cardiovascular mortality, and HF hospitalization for patients with preserved EF. More aggressive interventions targeting HFpEF in addition to the TAVI procedure might be relevant in patients with high H2FPEF scores, particularly in those with a lower surgical risk.
Keywords: Aortic stenosis; H2FPEF score; Heart failure; Long‐term outcomes; Preserved ejection fraction; Transcatheter aortic valve implantation.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
K.H., S.S., and N.T. are clinical proctors for Edwards Lifesciences, Medtronic, and Abbott Medical. M. Yamamoto, T.N., K.M., H.T., H.U., and Y.W. are clinical proctors for Edwards Lifesciences and Medtronic. K.T. is a clinical proctor for Edwards Lifesciences. F. Yashima is a clinical proctor for Medtronic. The remaining authors have nothing to disclose.
Figures
Similar articles
-
Heart Failure With Preserved Ejection Fraction Phenotype Is Associated With Early Symptom Onset in Aortic Stenosis and Residual Symptoms After Transcatheter Aortic Valve Implantation.J Am Heart Assoc. 2025 May 6;14(9):e038786. doi: 10.1161/JAHA.124.038786. Epub 2025 Apr 16. J Am Heart Assoc. 2025. PMID: 40240943 Free PMC article.
-
Prognostic value of the H2 FPEF score in patients undergoing transcatheter aortic valve implantation.ESC Heart Fail. 2021 Feb;8(1):461-470. doi: 10.1002/ehf2.13096. Epub 2020 Nov 20. ESC Heart Fail. 2021. PMID: 33215870 Free PMC article.
-
H2FPEF and HFA-PEFF scores for heart failure risk stratification in hypertrophic cardiomyopathy patients.ESC Heart Fail. 2025 Jun;12(3):2225-2238. doi: 10.1002/ehf2.15247. Epub 2025 Mar 1. ESC Heart Fail. 2025. PMID: 40022558 Free PMC article.
-
Meta-Analysis of the Prognostic Impact of Stroke Volume, Gradient, and Ejection Fraction After Transcatheter Aortic Valve Implantation.Am J Cardiol. 2015 Sep 15;116(6):989-94. doi: 10.1016/j.amjcard.2015.06.027. Epub 2015 Jun 26. Am J Cardiol. 2015. PMID: 26195275 Review.
-
Causes and Determinants of Heart Failure Readmissions Post Transcutaneous Aortic Valve Replacement: A Systematic Review and Meta-Analysis.Curr Probl Cardiol. 2023 Jan;48(1):101428. doi: 10.1016/j.cpcardiol.2022.101428. Epub 2022 Sep 30. Curr Probl Cardiol. 2023. PMID: 36191693
Cited by
-
Heart Failure With Preserved Ejection Fraction Phenotype Is Associated With Early Symptom Onset in Aortic Stenosis and Residual Symptoms After Transcatheter Aortic Valve Implantation.J Am Heart Assoc. 2025 May 6;14(9):e038786. doi: 10.1161/JAHA.124.038786. Epub 2025 Apr 16. J Am Heart Assoc. 2025. PMID: 40240943 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
