

Non-High-Density Lipoprotein Cholesterol Levels From Childhood to Adulthood and Cardiovascular Disease Events
- PMID: 38607340
- PMCID: PMC11151142
- DOI: 10.1001/jama.2024.4819
Non-High-Density Lipoprotein Cholesterol Levels From Childhood to Adulthood and Cardiovascular Disease Events
Abstract
Importance: Elevated non-high-density lipoprotein cholesterol (non-HDL-C; a recommended measure of lipid-related cardiovascular risk) is common in children and increases risk of adult cardiovascular disease (CVD). Whether resolution of elevated childhood non-HDL-C levels by adulthood is associated with reduced risk of clinical CVD events is unknown.
Objective: To examine the associations of non-HDL-C status between childhood and adulthood with incident CVD events.
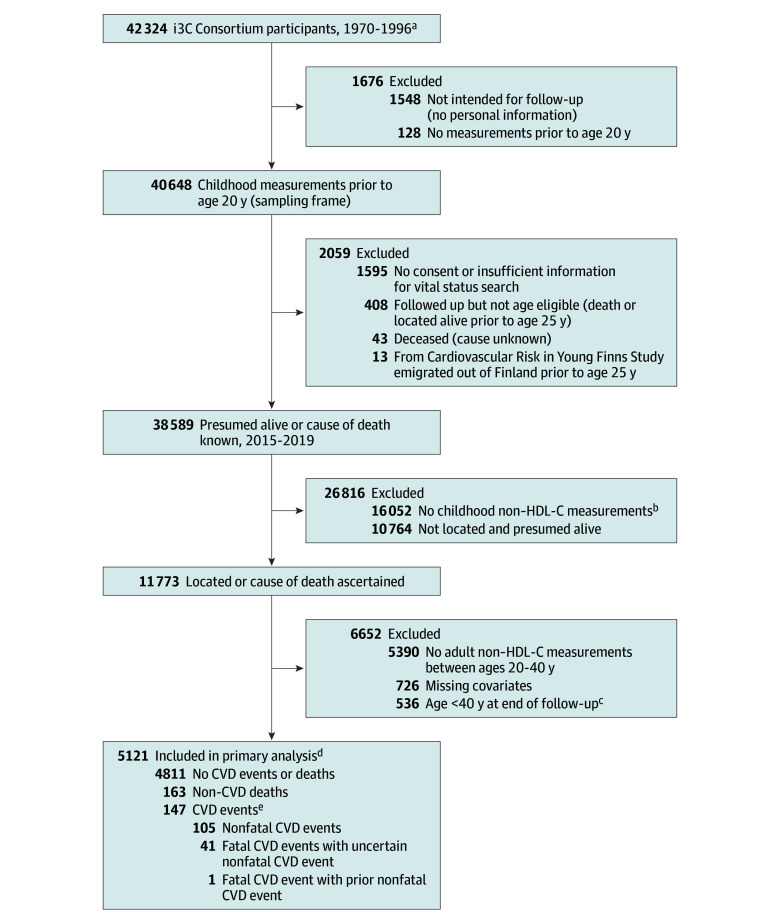
Design, setting, and participants: Individual participant data from 6 prospective cohorts of children (mean age at baseline, 10.7 years) in the US and Finland. Recruitment took place between 1970 and 1996, with a final follow-up in 2019.
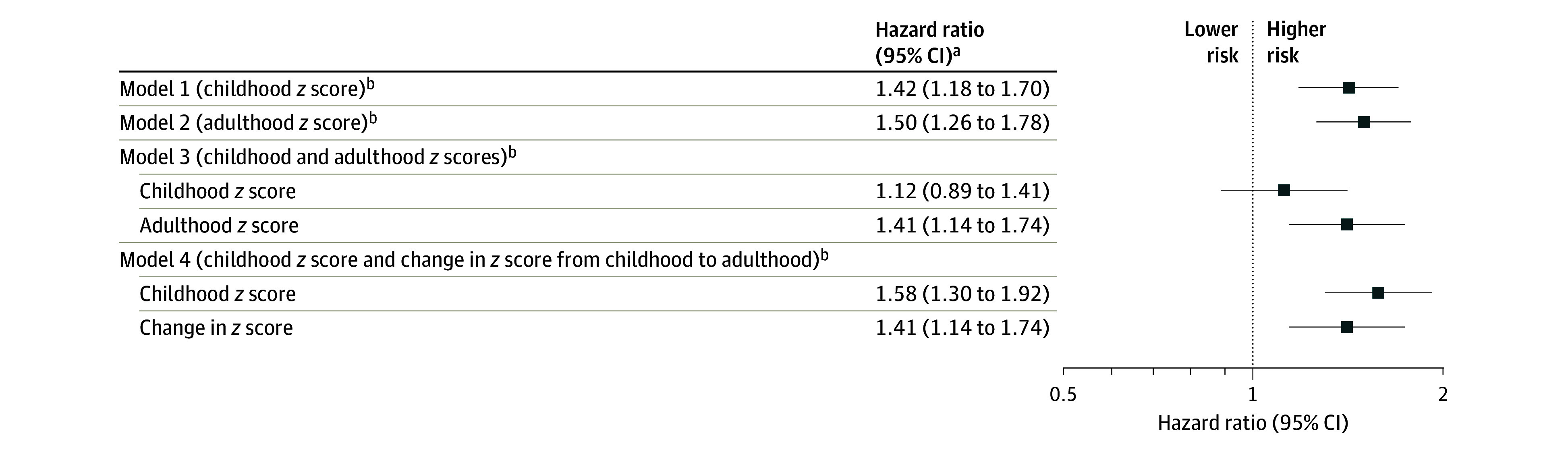
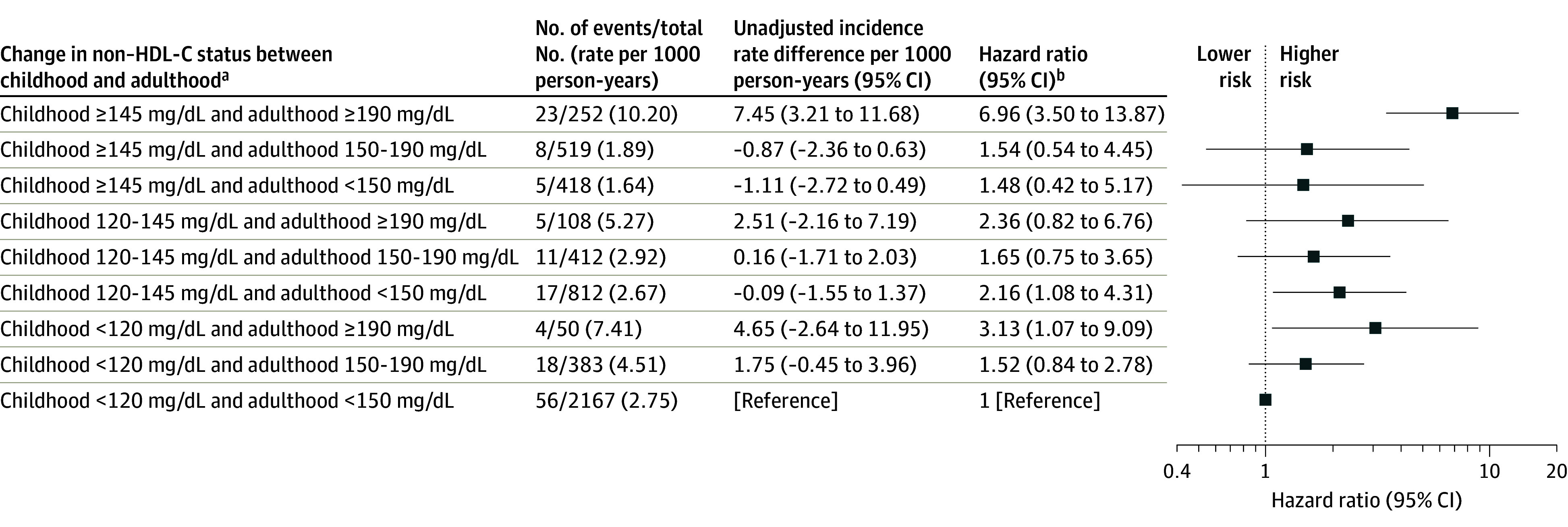
Exposures: Child (age 3-19 years) and adult (age 20-40 years) non-HDL-C age- and sex-specific z scores and categories according to clinical guideline-recommended cutoffs for dyslipidemia.
Main outcomes and measures: Incident fatal and nonfatal CVD events adjudicated by medical records.
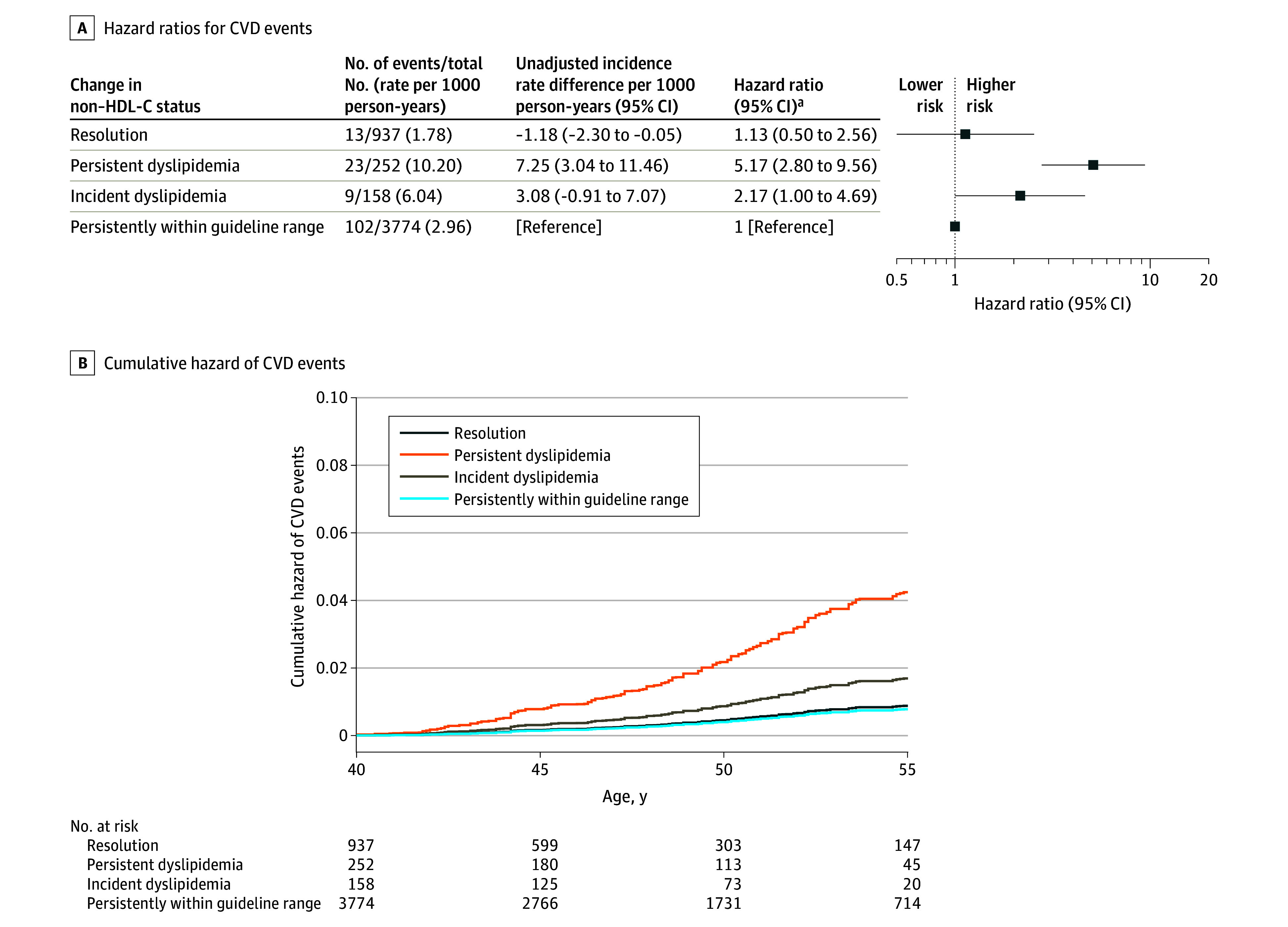
Results: Over a mean length of follow-up of 8.9 years after age 40 years, 147 CVD events occurred among 5121 participants (60% women; 15% Black). Both childhood and adult non-HDL-C levels were associated with increased risk of CVD events (hazard ratio [HR], 1.42 [95% CI, 1.18-1.70] and HR, 1.50 [95% CI, 1.26-1.78] for a 1-unit increase in z score, respectively), but the association for childhood non-HDL-C was reduced when adjusted for adult levels (HR, 1.12 [95% CI, 0.89-1.41]). A complementary analysis showed that both childhood non-HDL-C levels and the change between childhood and adulthood were independently associated with the outcome, suggesting that from a preventive perspective, both childhood non-HDL-C levels and the change into adulthood are informative. Compared with those whose non-HDL-C levels remained within the guideline-recommended range in childhood and adulthood, participants who had incident non-HDL-C dyslipidemia from childhood to adulthood and those with persistent dyslipidemia had increased risks of CVD events (HR, 2.17 [95% CI, 1.00-4.69] and HR, 5.17 [95% CI, 2.80-9.56], respectively). Individuals who had dyslipidemic non-HDL-C in childhood but whose non-HDL-C levels were within the guideline-recommended range in adulthood did not have a significantly increased risk (HR, 1.13 [95% CI, 0.50-2.56]).
Conclusions and relevance: Individuals with persistent non-HDL-C dyslipidemia from childhood to adulthood had an increased risk of CVD events, but those in whom dyslipidemic non-HDL-C levels resolve by adulthood have similar risk to individuals who were never dyslipidemic. These findings suggest that interventions to prevent and reduce elevated childhood non-HDL-C levels may help prevent premature CVD.
Conflict of interest statement
Figures
References
-
- Pahkala K, Laitinen TT, Niinikoski H, et al. Effects of 20-year infancy-onset dietary counselling on cardiometabolic risk factors in the Special Turku Coronary Risk Factor Intervention Project (STRIP): 6-year post-intervention follow-up. Lancet Child Adolesc Health. 2020;4(5):359-369. doi: 10.1016/S2352-4642(20)30059-6 - DOI - PubMed
-
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents . Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: summary report. Pediatrics. 2011;128(suppl 5):S213-S256. doi: 10.1542/peds.2009-2107C - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R33 AG057983/AG/NIA NIH HHS/United States
- R01 DK072124/DK/NIDDK NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- R01 HD032194/HD/NICHD NIH HHS/United States
- R01 HL048050/HL/NHLBI NIH HHS/United States
- RF1 AG041200/AG/NIA NIH HHS/United States
- R01 AG062309/AG/NIA NIH HHS/United States
- R03 HD062783/HD/NICHD NIH HHS/United States
- N01 HC055025/HC/NHLBI NIH HHS/United States
- R03 HD047247/HD/NICHD NIH HHS/United States
- R01 HL002942/HL/NHLBI NIH HHS/United States
- R01 HL121230/HL/NHLBI NIH HHS/United States
- R01 HL062394/HL/NHLBI NIH HHS/United States
- R01 HL034659/HL/NHLBI NIH HHS/United States
- R03 AG060619/AG/NIA NIH HHS/United States
- R01 HL052851/HL/NHLBI NIH HHS/United States
- R21 DK085363/DK/NIDDK NIH HHS/United States
- R01 HL054730/HL/NHLBI NIH HHS/United States
- R01 HL061857/HL/NHLBI NIH HHS/United States
- R01 AI176494/AI/NIAID NIH HHS/United States
- R01 AG016592/AG/NIA NIH HHS/United States
- R01 GM028719/GM/NIGMS NIH HHS/United States
- R01 HD069587/HD/NICHD NIH HHS/United States
- R01 HD029569/HD/NICHD NIH HHS/United States
- R01 ES021724/ES/NIEHS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
