

A case of multidrug-resistant intractable pylephlebitis and intra-abdominal abscess due to perforated appendicitis successfully treated with open abdominal management
- PMID: 38607465
- PMCID: PMC11014825
- DOI: 10.1186/s40792-024-01882-1
A case of multidrug-resistant intractable pylephlebitis and intra-abdominal abscess due to perforated appendicitis successfully treated with open abdominal management
Abstract
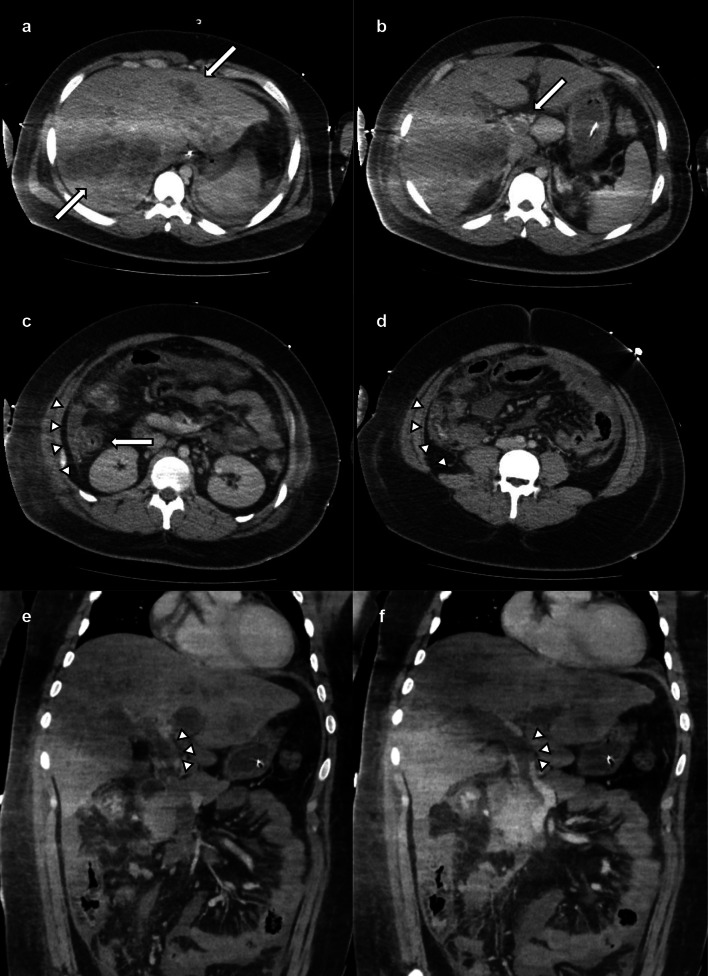
Background: Pylephlebitis, a rare and lethal form of portal venous septic thrombophlebitis, often arises from infections in regions drained by the portal vein. Herein, we report a case of peritonitis with portal vein thrombosis due to acute severe appendicitis, managed with intensive intraperitoneal drainage via open abdominal management (OAM).
Case presentation: A 19-year-old male with severe appendicitis, liver abscesses, and portal vein thrombosis developed septic shock and multi-organ failure. After emergency interventions, the patient was admitted to the intensive care unit. Antibiotic treatment based on cultures revealing multidrug-resistant Escherichia coli and Bacteroides fragilis and anticoagulation therapy (using heparin and edoxaban) was initiated. Despite continuous antibiotic therapy, the laboratory results consistently showed elevated levels of inflammatory markers. On the 13th day, open abdominal irrigation was performed for infection control. Extensive intestinal edema precluded wound closure, necessitating open-abdominal management in the intensive care unit. Anticoagulation therapy was continued, and intra-abdominal washouts were performed every 5 days. On the 34th day, wound closure was achieved using the anterior rectus abdominis sheath turnover method. The patient recovered successfully and was discharged on the 81st day.
Conclusions: Alongside appropriate antibiotic selection, early surgical drainage and OAM are invaluable. This case underscores the potential of anticoagulation therapy in facilitating safe surgical procedures.
Keywords: Acute severe appendicitis; Multidrug-resistant Bacteroides fragilis; Open abdominal management; Pylephlebitis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests associated with this manuscript.
Figures




References
-
- Singh P, Yadav N, Visvalingam V, Indaram A, Bank S. Pylephlebitis—diagnosis and management. Off J Am College Gastroenterol. 2001;96:1312–1313. - PubMed
-
- Shinji O, Ryosuke H, Tsuyoshi H, Okamoto T, Yanaga K. Portal vein thronmbosis caused by appendicitis successfully treates with conservative therapy -A c case report- J Jpn Surg Asssoc. 2013;74:3063–3067. doi: 10.3919/jjsa.74.3063. - DOI
LinkOut - more resources
Full Text Sources
