

An artificial intelligence-generated model predicts 90-day survival in alcohol-associated hepatitis: A global cohort study
- PMID: 38607809
- PMCID: PMC11798100
- DOI: 10.1097/HEP.0000000000000883
An artificial intelligence-generated model predicts 90-day survival in alcohol-associated hepatitis: A global cohort study
Abstract
Background and aims: Alcohol-associated hepatitis (AH) poses significant short-term mortality. Existing prognostic models lack precision for 90-day mortality. Utilizing artificial intelligence in a global cohort, we sought to derive and validate an enhanced prognostic model.
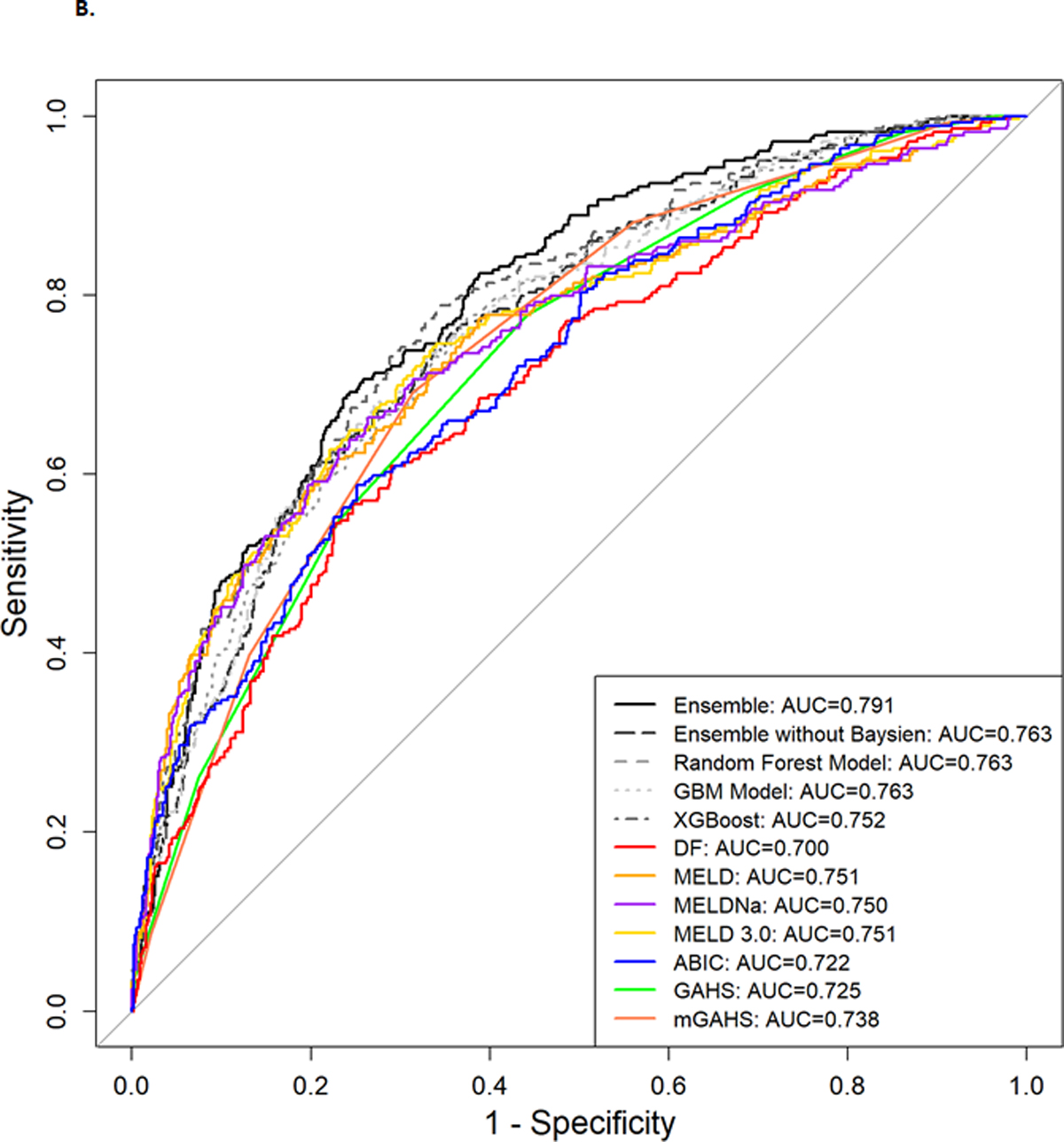
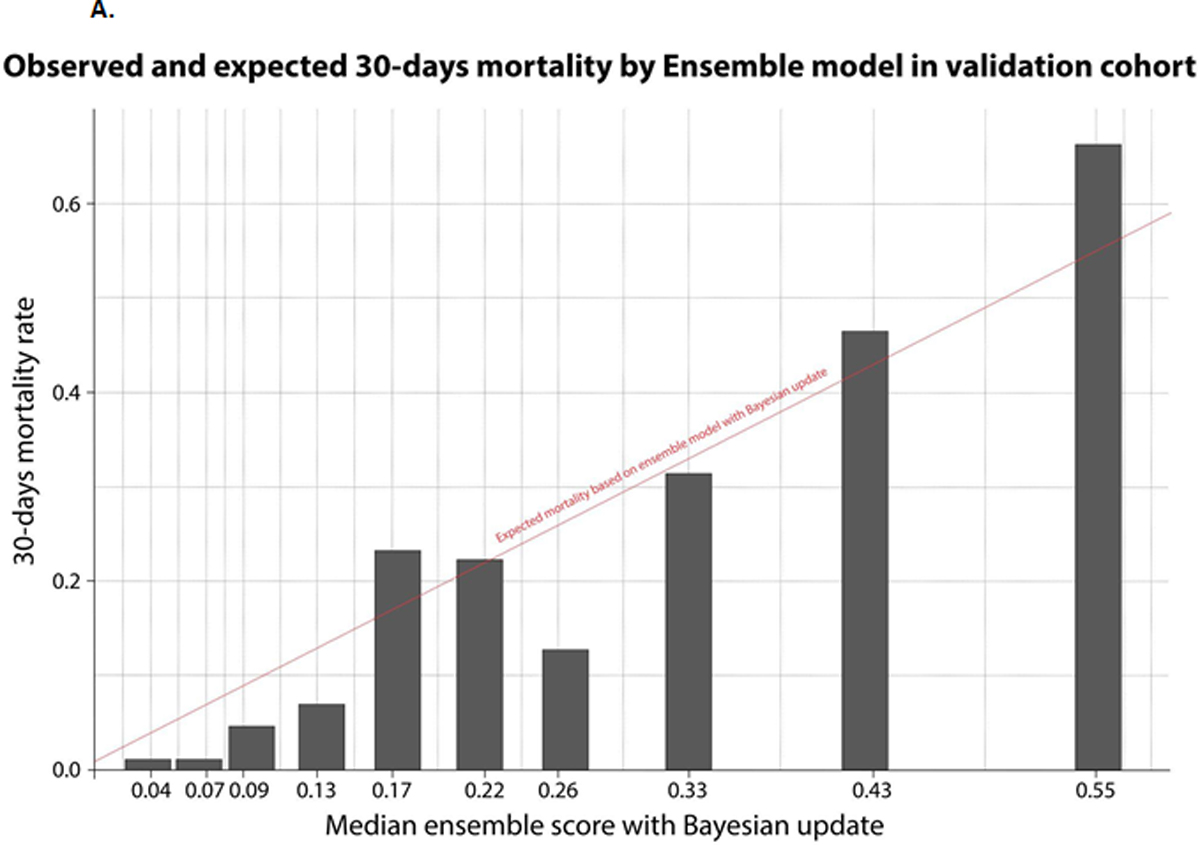
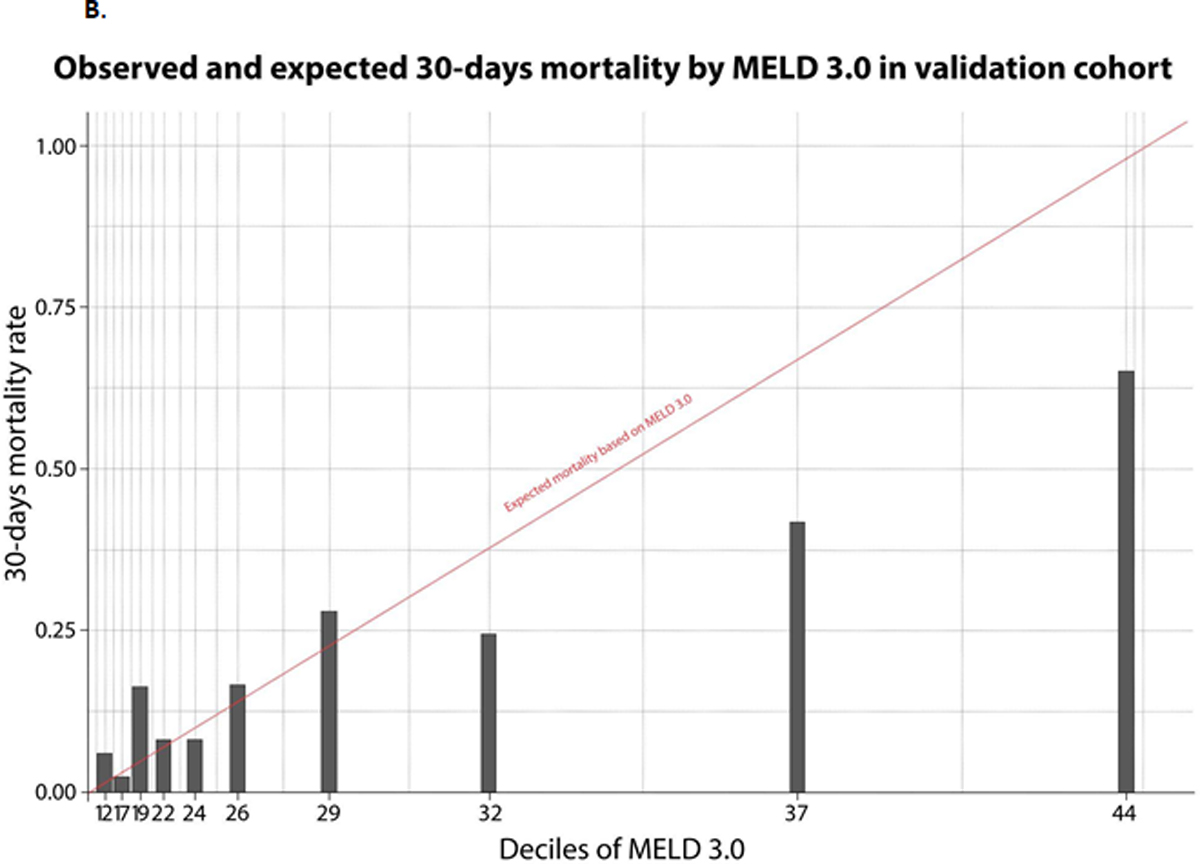
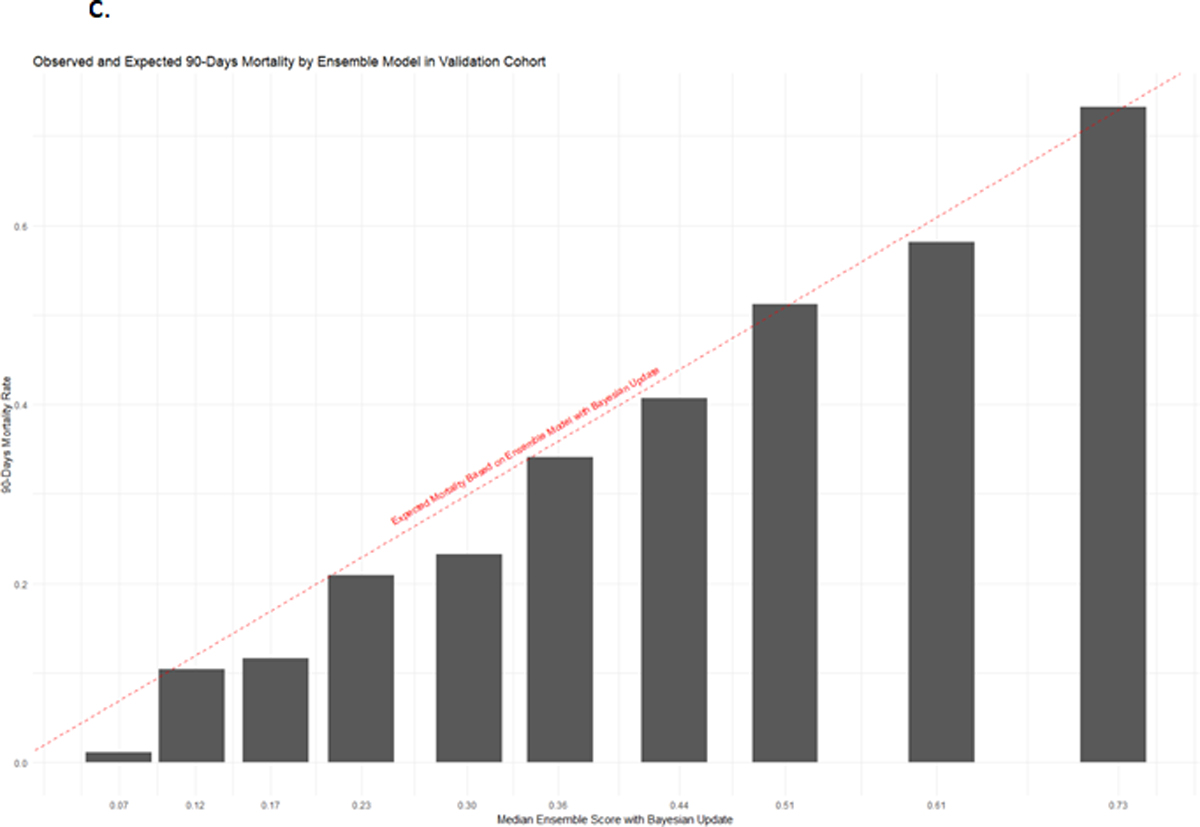
Approach and results: The Global AlcHep initiative, a retrospective study across 23 centers in 12 countries, enrolled patients with AH per National Institute for Alcohol Abuse and Alcoholism criteria. Centers were partitioned into derivation (11 centers, 860 patients) and validation cohorts (12 centers, 859 patients). Focusing on 30 and 90-day postadmission mortality, 3 artificial intelligence algorithms (Random Forest, Gradient Boosting Machines, and eXtreme Gradient Boosting) informed an ensemble model, subsequently refined through Bayesian updating, integrating the derivation cohort's average 90-day mortality with each center's approximate mortality rate to produce posttest probabilities. The ALCoholic Hepatitis Artificial INtelligence Ensemble score integrated age, gender, cirrhosis, and 9 laboratory values, with center-specific mortality rates. Mortality was 18.7% (30 d) and 27.9% (90 d) in the derivation cohort versus 21.7% and 32.5% in the validation cohort. Validation cohort 30 and 90-day AUCs were 0.811 (0.779-0.844) and 0.799 (0.769-0.830), significantly surpassing legacy models like Maddrey's Discriminant Function, Model for End-Stage Liver Disease variations, age-serum bilirubin-international normalized ratio-serum Creatinine score, Glasgow, and modified Glasgow Scores ( p < 0.001). ALCoholic Hepatitis Artificial INtelligence Ensemble score also showcased superior calibration against MELD and its variants. Steroid use improved 30-day survival for those with an ALCoholic Hepatitis Artificial INtelligence Ensemble score > 0.20 in both derivation and validation cohorts.
Conclusions: Harnessing artificial intelligence within a global consortium, we pioneered a scoring system excelling over traditional models for 30 and 90-day AH mortality predictions. Beneficial for clinical trials, steroid therapy, and transplant indications, it's accessible at: https://aihepatology.shinyapps.io/ALCHAIN/ .
Copyright © 2024 American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures




References
-
- Shirazi F, Singal AK, Wong RJ. Alcohol-associated Cirrhosis and Alcoholic Hepatitis Hospitalization Trends in the United States. J Clin Gastroenterol 2021;55:174–179. - PubMed
-
- Maddrey WC, Boitnott JK, Bedine MS, Weber FL Jr., Mezey E, White RI Jr. Corticosteroid therapy of alcoholic hepatitis. Gastroenterology 1978;75:193–199. - PubMed
-
- Dominguez M, Rincon D, Abraldes JG, et al. A new scoring system for prognostic stratification of patients with alcoholic hepatitis. Am J Gastroenterol 2008;103:2747–2756. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
