

Disparities in Teleneurology Use in Medicaid Beneficiaries With Epilepsy by Practice Setting: Promoting Health Equity in Academic Centers
- PMID: 38608210
- PMCID: PMC11175647
- DOI: 10.1212/WNL.0000000000209348
Disparities in Teleneurology Use in Medicaid Beneficiaries With Epilepsy by Practice Setting: Promoting Health Equity in Academic Centers
Abstract
Background and objectives: Medicaid beneficiaries in many American academic medical centers can receive care in a separate facility than those not covered by Medicaid. We aimed to identify possible disparities in care by evaluating the association between facility type (integrated faculty practice or Medicaid-only outpatient clinic) and telehealth utilization in people with epilepsy.
Methods: We performed retrospective analyses using structured data from the Mount Sinai Health System electronic medical record data from January 2003 to August 2021. We identified people of all ages with epilepsy who were followed by an epileptologist after January 3, 2018, using a validated ICD-9-CM/10-CM coded case definition. We evaluated associations between practice setting and telehealth utilization, an outcome measure that captures the evolving delivery of neurologic care in a post-coronavirus disease 2019 era, using multivariable logistic regression.
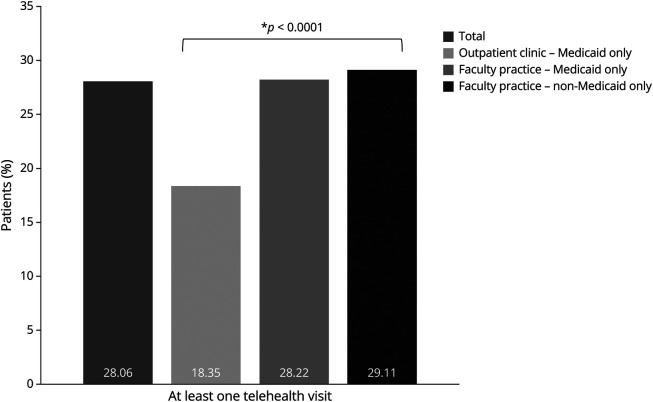
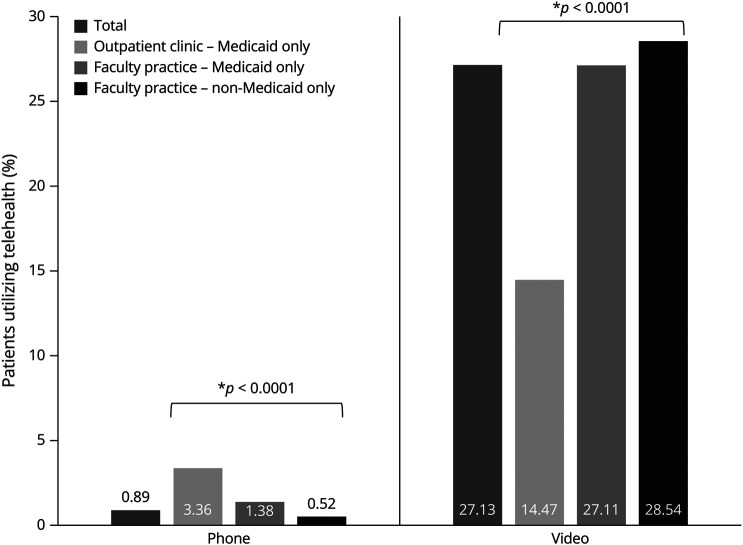
Results: We identified 4,586 people with epilepsy seen by an epileptologist, including Medicaid beneficiaries in the Medicaid outpatient clinic (N = 387), Medicaid beneficiaries in the faculty practice after integration (N = 723), and non-Medicaid beneficiaries (N = 3,476). Patients not insured by Medicaid were significantly older (average age 40 years vs 29 in persons seen in Medicaid-only outpatient clinic and 28.5 in persons insured with Medicaid seen in faculty practice [p < 0.0001]). Medicaid beneficiaries were more likely to have drug-resistant epilepsy (DRE), with 51.94% of people seen in Medicaid-only outpatient clinic, 41.63% of Medicaid beneficiaries seen in faculty practice, and 37.2% of non-Medicaid beneficiaries having DRE (p < 0.0001). Medicaid outpatient clinic patients were less likely to have telehealth visits (phone or video); 81.65% of patients in the Medicaid outpatient clinic having no telehealth visits vs 71.78% of Medicaid beneficiaries in the faculty practice and 70.89% of non-Medicaid beneficiaries (p < 0.0001). In an adjusted logistic regression analysis, Medicaid beneficiaries had lower odds (0.61; 95% CI 0.46-0.81) of using teleneurology compared with all patients seen in faculty practice (p = 0.0005).
Discussion: Compared with the Medicaid-only outpatient clinic, we found higher telehealth utilization in the integrated faculty practice with no difference by insurance status (Medicaid vs other). Integrated care may be associated with better health care delivery in people with epilepsy; thus, future research should examine its impact on other epilepsy-related outcomes.
Conflict of interest statement
E. Gotlieb and P. Agarwal report no disclosures relevant to the manuscript. L.J. Blank received research support from the American Epilepsy Society, Epilepsy Foundation, NORSE Institute, the Mount Sinai Claude D Pepper Older American Independence Center (5P30AG028741-11), and the Icahn School of Medicine Department of Neurology for work unrelated to this manuscript. C.-S. Kwon, M. Muxfeldt, and J. Young report no disclosures relevant to the manuscript. N. Jette received grant funding paid to her institution from the National Institute of Neurological Disorders and Stroke (NIH U24NS107201, NIH IU54NS100064, and NIH U24NS113849), the American Epilepsy Society and the NORSE Institute for work unrelated this manuscript. She receives an honorarium for her work as an Associate Editor of
Figures
Similar articles
-
Identifying Demographic Trends in the Use of Audio-Video and Audio-Only Telehealth by Arizona Medicaid Beneficiaries Before and During the COVID-19 Pandemic.J Gen Intern Med. 2025 Mar;40(4):764-772. doi: 10.1007/s11606-024-09196-6. Epub 2024 Nov 25. J Gen Intern Med. 2025. PMID: 39585578 Free PMC article.
-
Trends and disparities in telehealth use among Louisiana Medicaid beneficiaries with type 2 diabetes.Diabetes Obes Metab. 2023 Sep;25(9):2680-2688. doi: 10.1111/dom.15155. Epub 2023 Jun 20. Diabetes Obes Metab. 2023. PMID: 37340211
-
Use of Recommended Neurodiagnostic Evaluation Among Patients With Drug-Resistant Epilepsy.JAMA Neurol. 2024 May 1;81(5):499-506. doi: 10.1001/jamaneurol.2024.0551. JAMA Neurol. 2024. PMID: 38557864 Free PMC article.
-
The US Medicaid Program: Coverage, Financing, Reforms, and Implications for Health Equity.JAMA. 2022 Sep 20;328(11):1085-1099. doi: 10.1001/jama.2022.14791. JAMA. 2022. PMID: 36125468 Review.
-
Quality, Spending, Utilization, and Outcomes Among Dual-Eligible Medicare-Medicaid Beneficiaries in Integrated Care Programs: A Systematic Review.JAMA Health Forum. 2024 Jul 5;5(7):e242187. doi: 10.1001/jamahealthforum.2024.2187. JAMA Health Forum. 2024. PMID: 39028653 Free PMC article.
Cited by
-
American Epilepsy Society/International League Against Epilepsy-North America Joint Task Force for Epilepsy Health Care Disparities in the United States.Epilepsy Curr. 2025 Jun 9:15357597251342227. doi: 10.1177/15357597251342227. Online ahead of print. Epilepsy Curr. 2025. PMID: 40502806 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical