

Amyand's hernia with concurrent appendicitis: A case of interval laparoscopic herniorrhaphy and literature review
- PMID: 38608522
- PMCID: PMC11017271
- DOI: 10.1016/j.ijscr.2024.109601
Amyand's hernia with concurrent appendicitis: A case of interval laparoscopic herniorrhaphy and literature review
Abstract
Introduction and importance: Amyand's hernia with concurrent appendicitis is rare, with a reported incidence of 0.13 % of all inguinal hernias. This condition is challenging to diagnose and manage and no optimal treatment has been established.
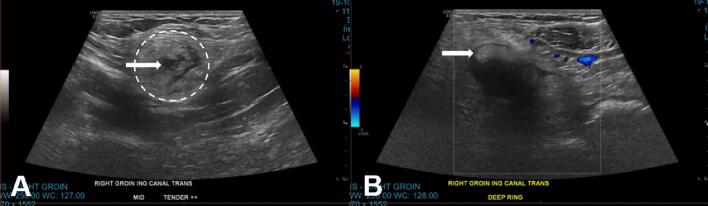
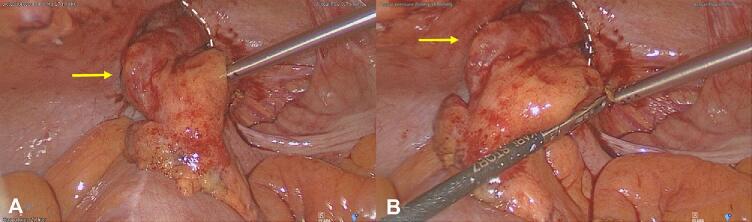
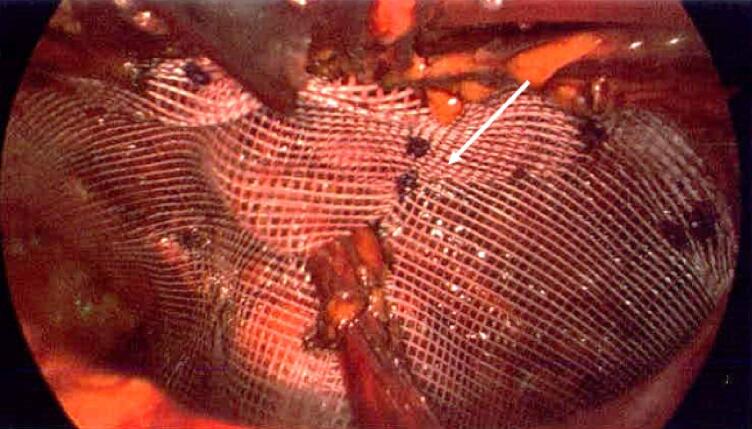
Case presentation: A 71-year-old man presented with an acutely painful, tender, and irreducible right inguinal hernia. He had a history of a right inguinal hernia for several months and had undergone open left inguinal hernia repair. The patient had no other medical comorbidities. Blood test results were nonspecific, with a C-reactive protein of 90 mg/L. Ultrasound scan suggested a strangulated right inguinal hernia. Laparoscopy revealed an Amyand's hernia with concurrent appendicitis and a pus-filled right inguinal hernia sac. The patient underwent laparoscopic appendicectomy, followed by staged laparoscopic transabdominal preperitoneal right inguinal hernia repair with mesh after eight weeks to reduce mesh infection. Histopathological examination confirmed acute uncomplicated appendicitis without perforation or malignancy. The patient had an unremarkable post-operative recovery.
Discussion: This case highlights the diagnostic challenges associated with Amyand's hernia and concurrent appendicitis. Laparoscopy provides both diagnostic and therapeutic opportunities. In this case, laparoscopic mesh herniorrhaphy was delayed and staged until local hernia sac inflammation resolved following appendicectomy.
Conclusion: Surgeons should have an index of suspicion for Amyand's hernia given the heterogeneity of presentations. A case-by-case approach is required to prevent post-operative complications and determine the safe timing of definitive hernia repair when the inguinal hernial sac is inflamed. Further research is required to provide surgeons with evidence-based approaches for this unique condition.
Keywords: Amyand's hernia; Appendicitis; Case report; Herniorrhaphy.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare no conflict of interest.
Figures
References
-
- Papaconstantinou D., Garoufalia Z., Kykalos S., Nastos C., Tsapralis D., Ioannidis O., et al. Implications of the presence of the vermiform appendix inside an inguinal hernia (Amyand’s hernia): a systematic review of the literature. Hernia. 2020;24:951–959. doi: 10.1007/s10029-020-02215-5. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
