

A novel combined approach to placement of a double lumen endobronchial tube using a video laryngoscope and fiberoptic bronchoscope: a retrospective chart review
- PMID: 38609865
- PMCID: PMC11010390
- DOI: 10.1186/s12871-024-02525-6
A novel combined approach to placement of a double lumen endobronchial tube using a video laryngoscope and fiberoptic bronchoscope: a retrospective chart review
Abstract
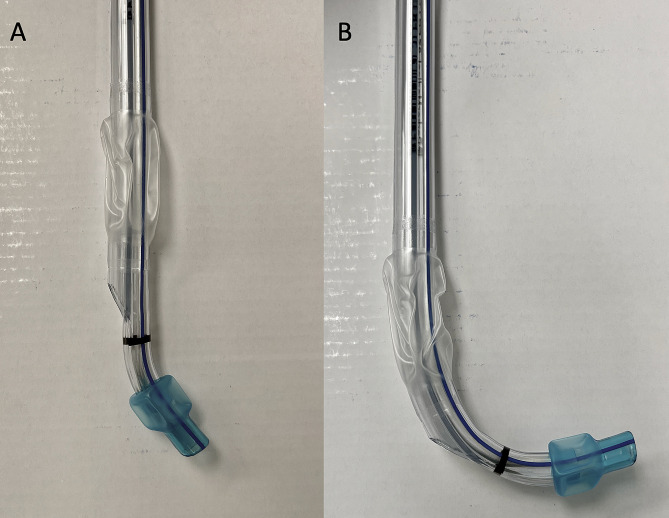
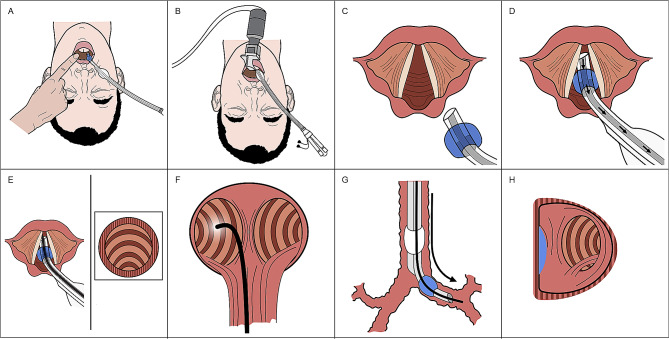
Background: The objective of this study was to evaluate a modern combined video laryngoscopy and flexible fiberoptic bronchoscope approach to placement of a double lumen endobronchial tube and further characterize potential strengths and weaknesses of this approach.
Methods: Retrospective chart review was conducted at our single institution, academic medical center, tertiary-care hospital. Patients aged 18 years of age or older were evaluated who underwent thoracic surgery and one-lung ventilation with placement of a double lumen endobronchial tube using a novel combined video laryngoscopy and flexible fiberoptic bronchoscope approach. No interventions were performed.
Results: Demographics and induction and intubation documentation were reviewed for 21 patients who underwent thoracic surgery and one-lung ventilation with placement of a double lumen endobronchial tube using a novel combined video laryngoscopy and flexible fiberoptic bronchoscope approach. First pass success using the combined approach was 86% (18/21). The five patients with an anticipated difficult airway had successful double lumen endobronchial tube placement on the first attempt. There were no instances of desaturation during double lumen endobronchial tube placement. No airway complications related to double lumen endobronchial tube placement were recorded.
Conclusion: Use of a combined approach employing video laryngoscopy and a flexible fiberoptic bronchoscope may represent a reliable alternative approach to placement of double lumen endobronchial tubes.
Keywords: Airway management; Double lumen endobronchial tube; One-lung ventilation; Thoracic anesthesia.
© 2024. The Author(s).
Conflict of interest statement
Founder of Pneuomocyte LLC. LM is now a paid consultant for Verathon the manufacturer of the Glidescope. He began his role as a consultant after the conclusion of this study and did not receive any funding during the time in which these cases occurred. LM has not previously been a consultant for Verathon. No other listed authors have any relevant competing interests.
Figures
References
-
- Lenhardt R, Burkhart MT, Brock GN, Kanchi-Kandadai S, Sharma R, Akça O. Is video laryngoscope-assisted flexible tracheoscope intubation feasible for patients with predicted difficult airway? A prospective, randomized clinical trial. Anesth Analg. 2014;118:1259–65. doi: 10.1213/ANE.0000000000000220. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
