

Non-traumatic osteonecrosis of the femoral head induced by steroid and alcohol exposure is associated with intestinal flora alterations and metabolomic profiles
- PMID: 38609952
- PMCID: PMC11015587
- DOI: 10.1186/s13018-024-04713-z
Non-traumatic osteonecrosis of the femoral head induced by steroid and alcohol exposure is associated with intestinal flora alterations and metabolomic profiles
Abstract
Objective: Osteonecrosis of the femoral head (ONFH) is a severe disease that primarily affects the middle-aged population, imposing a significant economic and social burden. Recent research has linked the progression of non-traumatic osteonecrosis of the femoral head (NONFH) to the composition of the gut microbiota. Steroids and alcohol are considered major contributing factors. However, the relationship between NONFH caused by two etiologies and the microbiota remains unclear. In this study, we examined the gut microbiota and fecal metabolic phenotypes of two groups of patients, and analyzed potential differences in the pathogenic mechanisms from both the microbial and metabolic perspectives.
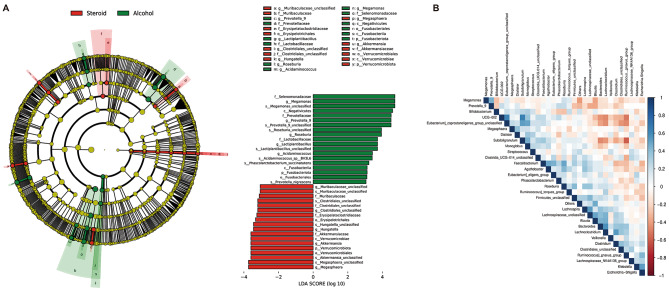
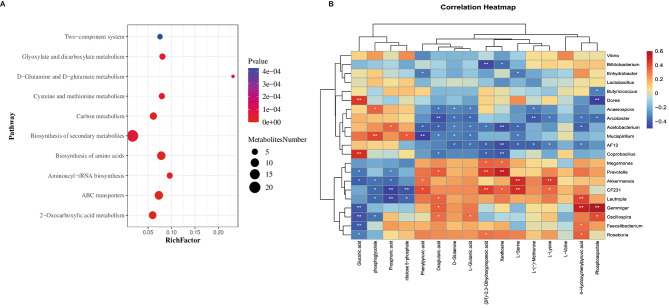
Methods: Utilizing fecal samples from 68 NONFH patients (32 steroid-induced, 36 alcohol-induced), high-throughput 16 S rDNA sequencing and liquid chromatography with tandem mass spectrometry (LC-MS/MS) metabolomics analyses were conducted. Univariate and multivariate analyses were applied to the omics data, employing linear discriminant analysis effect size to identify potential biomarkers. Additionally, functional annotation of differential metabolites and associated pathways was performed using the Kyoto Encyclopedia of Genes and Genomes (KEGG) database. Subsequently, Spearman correlation analysis was employed to assess the potential correlations between differential gut microbiota and metabolites.
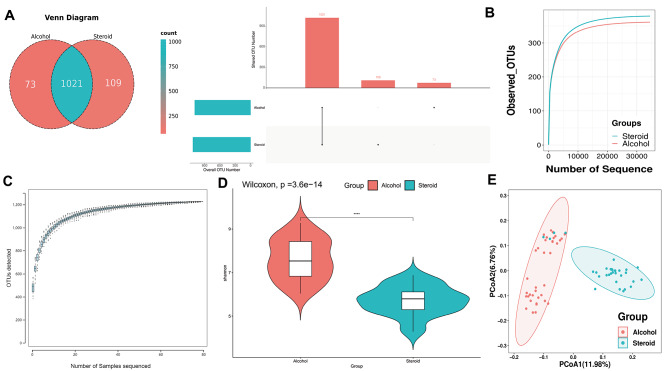
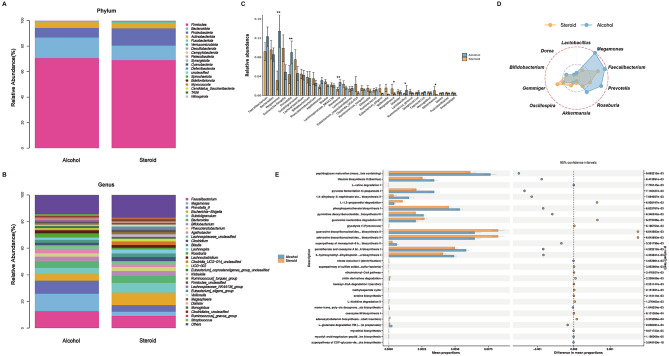
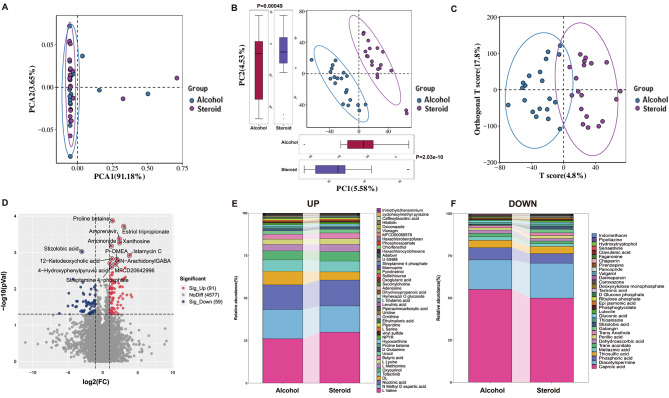
Results: High-throughput 16 S rDNA sequencing revealed significant gut microbial differences. At the genus level, the alcohol group had higher Lactobacillus and Roseburia, while the steroid group had more Megasphaera and Akkermansia. LC-MS/MS metabolomic analysis indicates significant differences in fecal metabolites between steroid- and alcohol-induced ONFH patients. Alcohol-induced ONFH (AONFH) showed elevated levels of L-Lysine and Oxoglutaric acid, while steroid-induced ONFH(SONFH) had increased Gluconic acid and Phosphoric acid. KEGG annotation revealed 10 pathways with metabolite differences between AONFH and SONFH patients. Correlation analysis revealed the association between differential gut flora and differential metabolites.
Conclusions: Our results suggest that hormones and alcohol can induce changes in the gut microbiota, leading to alterations in fecal metabolites. These changes, driven by different pathways, contribute to the progression of the disease. The study opens new research directions for understanding the pathogenic mechanisms of hormone- or alcohol-induced NONFH, suggesting that differentiated preventive and therapeutic approaches may be needed for NONFH caused by different triggers.
Keywords: Alcohol; Intestinal flora; Metabolomic profiles; Non-traumatic femoral head necrosis; Steroid.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
- Z211100002921046/The Beijing Science and Technology Planning Project
- Z211100002921046/The Beijing Science and Technology Planning Project
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
- 2020YFC2007405/The National key Research and Development Plan of the Ministry of Science and Technology of China
LinkOut - more resources
Full Text Sources
