

The effect of an anti-malarial herbal remedy, Maytenus senegalensis, on electrocardiograms of healthy Tanzanian volunteers
- PMID: 38609987
- PMCID: PMC11015626
- DOI: 10.1186/s12936-024-04935-w
The effect of an anti-malarial herbal remedy, Maytenus senegalensis, on electrocardiograms of healthy Tanzanian volunteers
Abstract
Background: The emergence of resistance to artemisinin-based combination therapy necessitates the search for new, more potent antiplasmodial compounds, including herbal remedies. The whole extract of Maytenus senegalensis has been scientifically investigated for potential biological activities both in vitro and in vivo, demonstrating strong antimalarial activity. However, there is a lack of data on the electrocardiographic effects of M. senegalensis in humans, which is a crucial aspect in the investigation of malaria treatment. Assessing the electrocardiographic effects of M. senegalensis is essential, as many anti-malarial drugs can inadvertently prolong the QT interval on electrocardiograms. Therefore, the study's objective was to evaluate the electrocardiographic effects of M. senegalensis in healthy adult volunteers.
Methods: This study is a secondary analysis of an open-label single-arm dose escalation. Twelve healthy eligible Tanzanian males, aged 18 to 45, were enrolled in four study dose groups. A single 12-lead electrocardiogram (ECG) was performed at baseline and on days 3, 7, 14, 28, and 56.
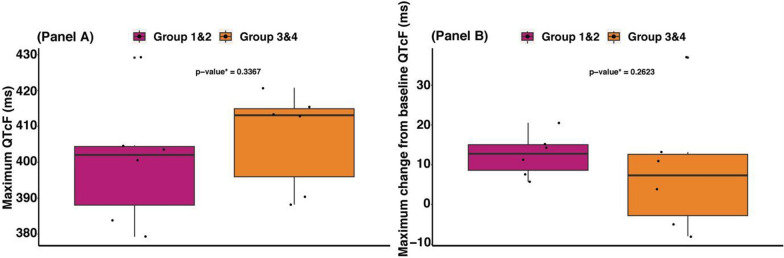
Results: No QTcF adverse events occurred with any drug dose. Only one volunteer who received the highest dose (800 mg) of M. senegalensis experienced a moderate transient change (△QTcF > 30 ms; specifically, the value was 37 ms) from baseline on day 28. There was no difference in maximum QTcF and maximum △QTcF between volunteers in all four study dose groups.
Conclusions: A four-day regimen of 800 mg every 8 h of M. senegalensis did not impact the electrocardiographic parameters in healthy volunteers. This study suggests that M. senegalensis could be a valuable addition to malaria treatment, providing a safer alternative and potentially aiding in the battle against artemisinin-resistant malaria. The results of this study support both the traditional use and the modern therapeutic potential of M. senegalensis. They also set the stage for future research involving larger and more diverse populations to explore the safety profile of M. senegalensis in different demographic groups. This is especially important considering the potential use of M. senegalensis as a therapeutic agent and its widespread utilization as traditional medicine. Trial registration ClinicalTrials.gov, NCT04944966. Registered 30 June 2021-Retrospectively registered, https://clinicaltrials.gov/ct2/show/NCT04944966?term=kamaka&draw=2&rank=1.
Keywords: M. senegalensis; Electrocardiographic effects; Healthy volunteer; Herbal remedy.
© 2024. The Author(s).
Conflict of interest statement
All authors declare that they have no commercial or other associations that may pose a conflict of interest.
Figures

References
-
- WHO . World malaria report 2023. Geneva: World Health Organization; 2023.
-
- WHO . Global technical strategy for malaria 2016–2030. Geneva: World Health Organization; 2015.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
