

The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience
- PMID: 38610810
- PMCID: PMC11012750
- DOI: 10.3390/jcm13072045
The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience
Abstract
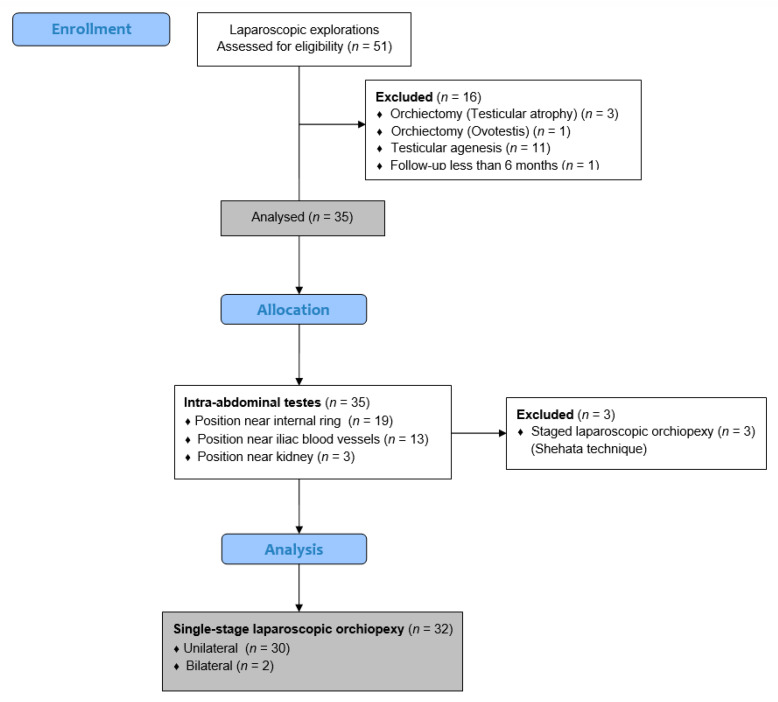
Objectives: Intra-abdominal testes are located in a variety of intra-abdominal positions, most less than 2 cm from the internal ring. Various surgical techniques of laparoscopic orchiopexy have been described to date. The aim of this study was to evaluate the safety and long-term efficacy of a single-stage, vessel-preserving, laparoscopic orchiopexy for intra-abdominal testes in pediatric patients. Methods: A retrospective search of the medical records of 32 children (34 testes) who underwent single-stage, vessel preserving, laparoscopic orchiopexy for intra-abdominal testes between 1 January 2014 and 31 December 2023 was performed. Single-stage laparoscopic orchiopexies were performed in all patients for whom sufficient length of the spermatic cord was achieved during the procedure. The volume of each patient's testes was measured using ultrasound before and 6 months after laparoscopic orchiopexy. The main outcome of this study was testicular volume before and after the procedure. The secondary outcomes were the occurrence of early and late complications, the duration of surgery, and the length of hospital stay. Results: The median age at the time of surgery was 10 months (interquartile range-IQR 9, 13). The majority of the children (n = 24; 75%) were less than 12 months old at the time of surgery. A normal testis was found in 24 patients (70.6%), while a hypotrophic testis was visible in 10 cases (29.4%). The majority of the testes were located near the internal ring (n = 19; 55.9%), while in the remaining cases, the testes were located near the iliac blood vessels. The median duration of the surgical procedure was 37.5 min (IQR 33, 42.5). The duration of hospitalization was one day for all the children. No intraoperative complications were observed. One child had a wound infection at the site of the umbilical trocar, which was treated conservatively. In two cases (5.5%), testicular atrophy was detected during long-term follow-up. In three cases, the testis was found in a higher position in the scrotum during the follow-up period, but in two cases, the position was normal during the follow-up period, while in one case, the position in the scrotum remained unchanged. At long-term follow-up with a median of 35 months (IQR 19, 60.5), the overall success rate was 94.5%. The median testicular volume at 6-month follow-up increased from 0.31 mL (IQR 0.28, 0.43) to 0.40 mL (IQR 0.33, 0.53) (p = 0.017). Conclusions: Single-stage, vessel-preserving, laparoscopic orchiopexies for intra-abdominal testes are safe and effective in pediatric patients in whom adequate spermatic cord length can be achieved during the procedure.
Keywords: children; cryptorchidism; intra-abdominal testis; laparoscopic orchiopexy; single-stage orchiopexy; vessels preserving orchiopexy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Staged laparoscopic orchiopexy of intra-abdominal testis: Spermatic vessels division versus traction? A multicentric comparative study.J Pediatr Urol. 2024 Jun;20(3):498.e1-498.e8. doi: 10.1016/j.jpurol.2024.01.017. Epub 2024 Jan 19. J Pediatr Urol. 2024. PMID: 38310033
-
Single setting bilateral laparoscopic orchiopexy for bilateral intra-abdominal testicles.J Urol. 2008 Oct;180(4 Suppl):1795-9; discussion 1799. doi: 10.1016/j.juro.2008.03.108. Epub 2008 Aug 21. J Urol. 2008. PMID: 18721983
-
Laparoscopic orchiopexy for a nonpalpable testis.Korean J Urol. 2010 Feb;51(2):106-10. doi: 10.4111/kju.2010.51.2.106. Epub 2010 Feb 18. Korean J Urol. 2010. PMID: 20414422 Free PMC article.
-
Splenogonadal fusion: a case report and review of the literature.BMC Urol. 2021 Feb 3;21(1):16. doi: 10.1186/s12894-021-00781-z. BMC Urol. 2021. PMID: 33536002 Free PMC article. Review.
-
Surgical Management of the Undescended Testis: Recent Advances and Controversies.Eur J Pediatr Surg. 2016 Oct;26(5):418-426. doi: 10.1055/s-0036-1592197. Epub 2016 Sep 15. Eur J Pediatr Surg. 2016. PMID: 27631723 Review.
Cited by
-
Development and validation of a predictive model for testicular atrophy after orchiopexy in children with testicular torsion.World J Emerg Med. 2025 Jul 1;16(4):387-391. doi: 10.5847/wjem.j.1920-8642.2025.079. World J Emerg Med. 2025. PMID: 40708733 Free PMC article. No abstract available.
References
-
- Pogorelić Z., Neumann C., Jukic M. An unusual presentation of testicular torsion in children: A single-centre retrospective study. Can. J. Urol. 2019;26:10026–10032. - PubMed
LinkOut - more resources
Full Text Sources
