

Clinical Trajectory and Risk Stratification for Heart Failure with Preserved Ejection Fraction in a Real-World Cohort of Patients with Suspected Coronary Artery Disease
- PMID: 38610857
- PMCID: PMC11012700
- DOI: 10.3390/jcm13072092
Clinical Trajectory and Risk Stratification for Heart Failure with Preserved Ejection Fraction in a Real-World Cohort of Patients with Suspected Coronary Artery Disease
Abstract
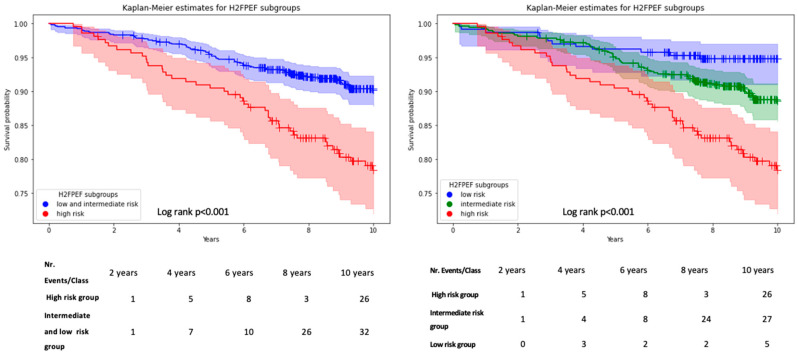
Background: Heart failure with preserved ejection fraction (HFpEF) is a widespread condition with significant morbidity and mortality. Its clinical heterogeneity may delay the diagnosis. Aim: To identify predictors of HFpEF-related hospitalizations in ambulatory patients presenting with elevated cardiovascular risk, suspected coronary artery diseases (CADs), and positive HFpEF screenings. Methods: Consecutive patients presenting with suspected CAD, enrolled in the observational LIFE-Heart study (2006-2014, NCT00497887), and meeting HFpEF criteria per the 2016 European Society of Cardiology (ESC) guidelines were categorized according to the presence of "overlapping conditions" potentially masking or contributing to their symptoms. Additional stratification using the H2FPEF score (<2: low risk, 2-5: intermediate risk, and ≥6 high risk) was performed. Follow-up for hospitalizations, reasons of hospitalization, and death spanned a median of 6 years. Results: Of 1054 patients (66 ± 10 years, 60% male, NT-pro-BNP 286, IQR 183-574 pg/mL), 53% had overlapping conditions, while 47% had "isolated HFpEF". The H2FPEF scores classified 23%, 57%, and 20% as low-, intermediate-, and high-risk, respectively, with consistent proportions across patients with and without overlapping conditions (p = 0.91). During the follow-up observational phase, 54% were rehospitalized, 22% experienced heart failure (HF) rehospitalizations, and 11% of patients died. Multivariable logistic regression revealed a high-risk H2FPEF category as an independent predictor of HF rehospitalization in the overall cohort (odds ratio: 3.4, CI: 2.4-4.9, p < 0.01) as well as in patients with and without overlapping conditions. Furthermore, a H2FPEF score ≥ 6 was independently associated with higher mortality rates (hazard ratio: 1.8, CI: 1.2-2.6, p < 0.01) in the Cox regression analysis. Conclusions: Ambulatory patients presenting for suspected CAD and meeting HFpEF screening criteria face elevated risks for rehospitalizations over six years. Regardless of concomitant diagnoses, quantifying cardiac damage with the H2FPEF score helps in risk-stratifying patients for HF hospitalization and mortality.
Keywords: H2FPEF score; coronary artery disease; heart failure hospitalization; heart failure with preserved ejection fraction.
Conflict of interest statement
Karl-Patrik Kresoja received travel grants from Edwards Lifesciences; Markus Scholz received funding from Pfizer Inc. for a project not related to this research. Markus Scholz also receives funding from Owkin for providing data of HFpEF patients. The company had no impact on the research activities of the group nor the interpretation of results; Berend Isermann is member of the Scientific Advisory Board of Function, Therapeutics, Inc. and received an unrestricted research funds from Aplagon Oy, Finland.
Figures


References
-
- Sanderson J.E. Heart Failure with a Normal Ejection Fraction. [(accessed on 13 June 2016)];Heart. 2007 93:155–158. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16387829. - PMC - PubMed
-
- Nair N. Epidemiology and pathogenesis of heart failure with preserved ejection fraction. Rev. Cardiovasc. Med. 2020;21:531–540. - PubMed
-
- Borlaug B.A., Paulus W.J. Heart Failure with Preserved Ejection Fraction: Pathophysiology, Diagnosis, and Treatment. [(accessed on 13 June 2016)];Eur. Heart J. 2011 32:670–679. doi: 10.1093/eurheartj/ehq426. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21138935. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
