

Rationale for Using High-Frequency Ultrasound as a Routine Examination in Skin Cancer Surgery: A Practical Approach
- PMID: 38610917
- PMCID: PMC11012407
- DOI: 10.3390/jcm13072152
Rationale for Using High-Frequency Ultrasound as a Routine Examination in Skin Cancer Surgery: A Practical Approach
Abstract
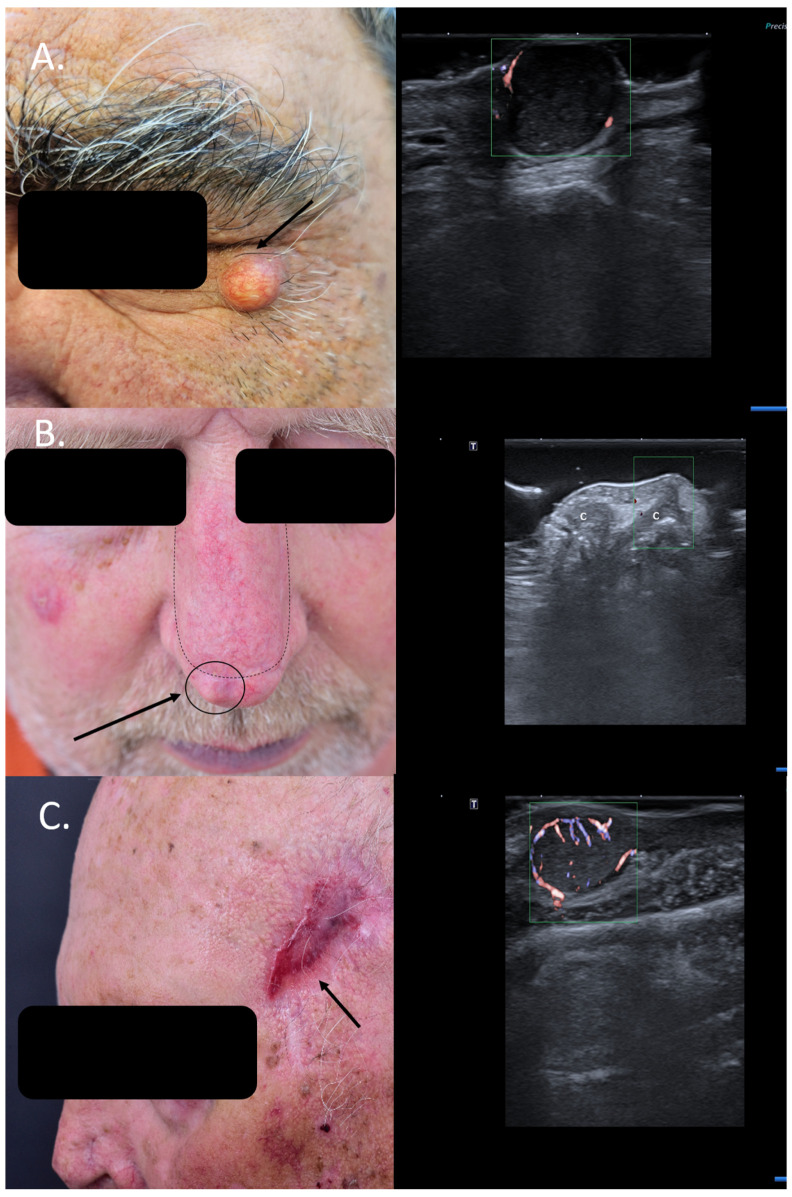
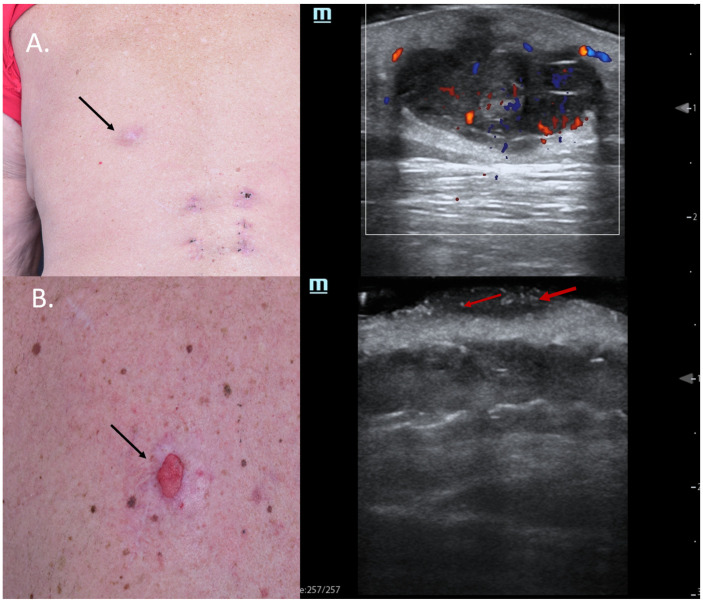
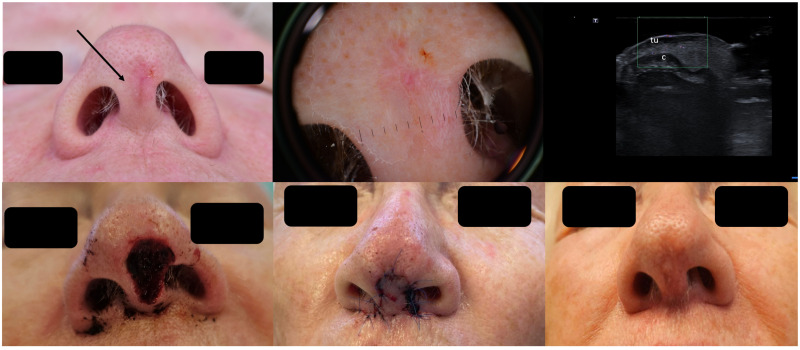
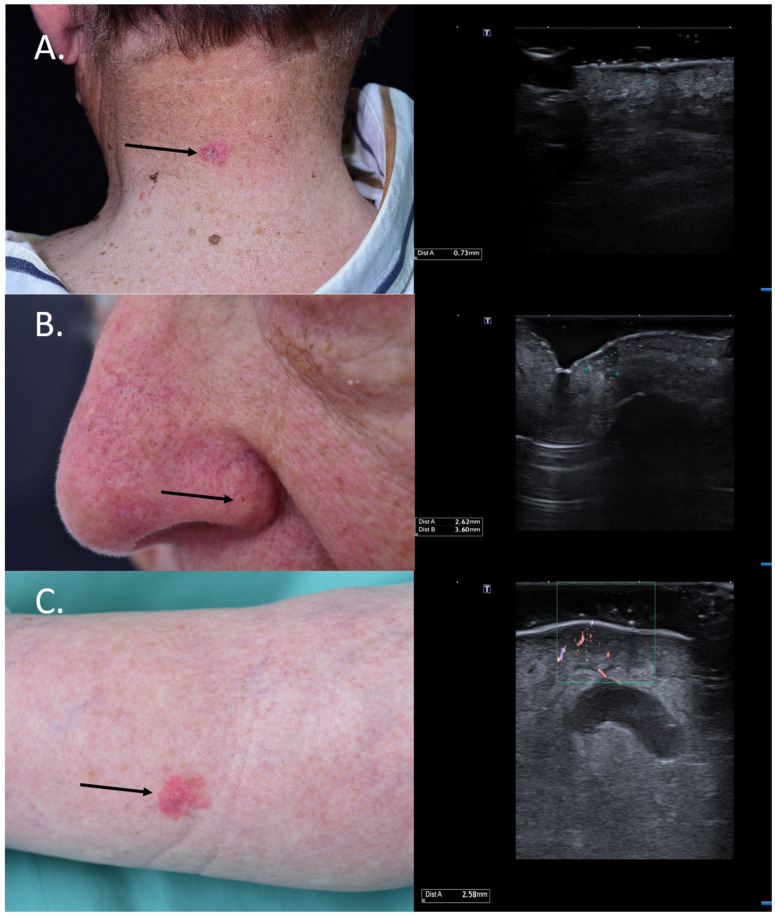
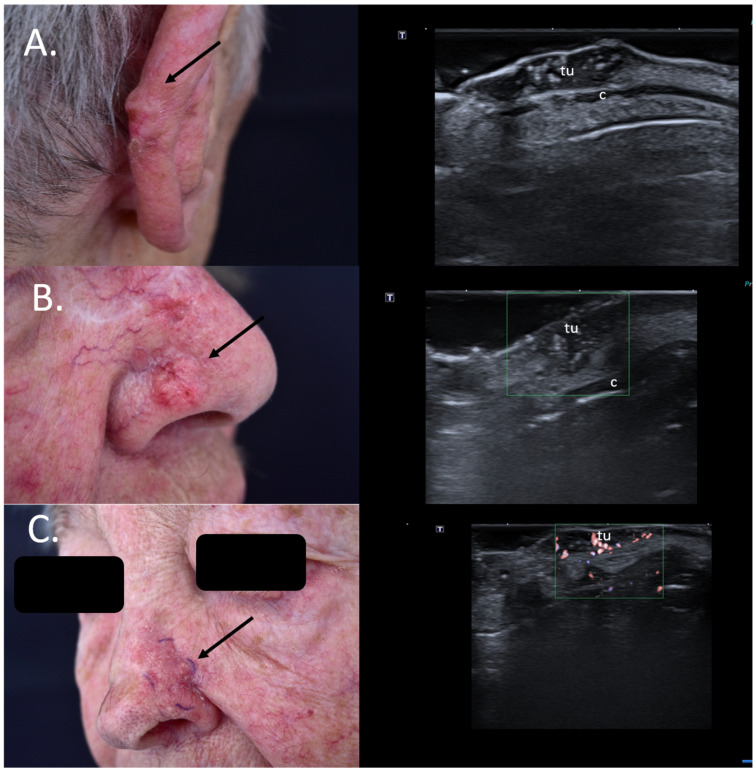
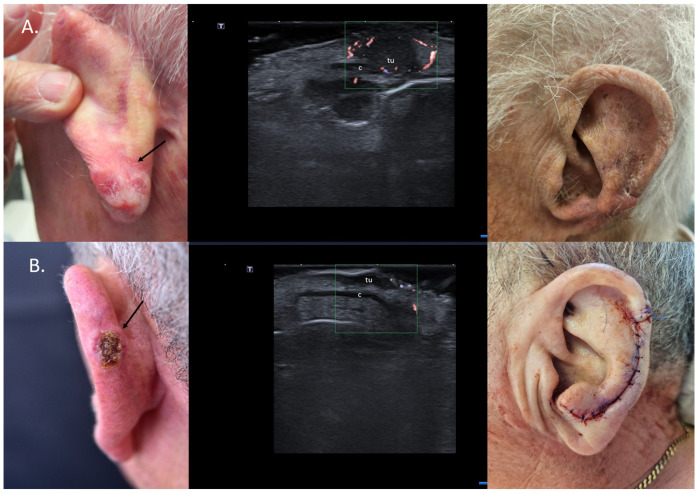
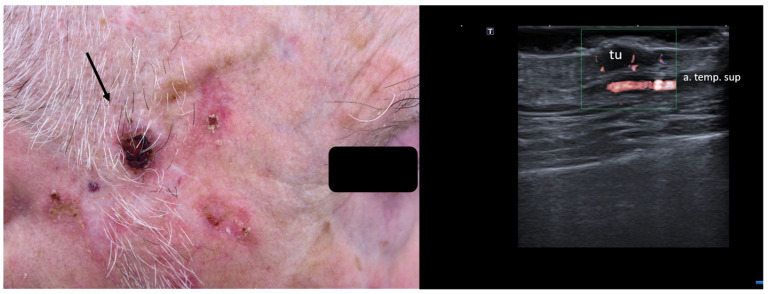
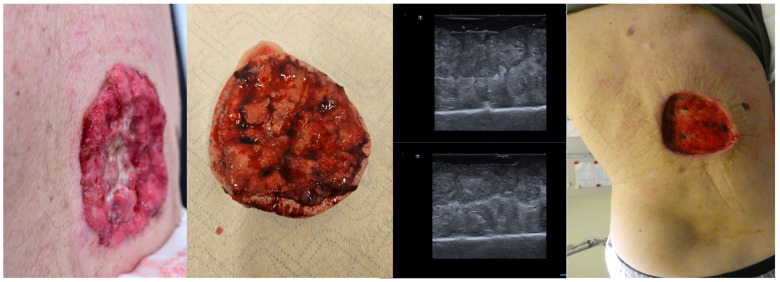
Ultrasound and high-frequency ultrasound assessment of melanoma and non-melanoma skin cancer in the pre-therapeutical setting is becoming increasingly popular in the field of dermatosurgery and dermatooncology, as it can provide clinicians with relevant, "in vivo" parameters regarding tumor lateral and depth extension as well as potential locoregional spread, cancelling the need of more extensive imaging methods and avoiding a delay in diagnosis. Furthermore, preoperative sonography and color Doppler can aid in orienting the clinical diagnosis, being able in numerous situations to differentiate between benign and malignant lesions, which require a different therapeutic approach. This preoperative knowledge is of paramount importance for planning an individualized treatment regimen. Using sonography at the time of diagnosis, important surgical complications, such as neurovascular damage, can be avoided by performing a preoperative neurovascular mapping. Furthermore, sonography can help reduce the number of surgical steps by identifying the lesions' extent prior to surgery, but it can also spare unnecessary surgical interventions in cases of locally advanced lesions, which infiltrate the bone or already present with locoregional metastases, which usually require modern radiooncological therapies in accordance to European guidelines. With this review, we intend to summarize the current indications of sonography in the field of skin cancer surgery, which can help us improve the therapeutic attitude toward our patients and enhance patient counseling. In the era of modern systemic radiooncological therapies, sonography can help better select patients who qualify for surgical procedures or require systemic treatments due to tumoral extension.
Keywords: dermatosurgery; malignant melanoma; non-melanoma skin cancer; skin cancer; ultrasound.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Ultrasonographic Assessment of Depth Infiltration in Melanoma and Non-melanoma Skin Cancer.J Ultrasound Med. 2023 Jul;42(7):1609-1616. doi: 10.1002/jum.16180. Epub 2023 Jan 30. J Ultrasound Med. 2023. PMID: 36714967
-
Pre-operative high-frequency ultrasound: a reliable management tool in auricular and nasal non-melanoma skin cancer.J Dtsch Dermatol Ges. 2024 Mar;22(3):357-365. doi: 10.1111/ddg.15308. Epub 2024 Jan 20. J Dtsch Dermatol Ges. 2024. PMID: 38243870
-
Ultrasonography in dermatologic surgery: revealing the unseen for improved surgical planning.J Dtsch Dermatol Ges. 2022 Jul;20(7):913-926. doi: 10.1111/ddg.14781. Epub 2022 May 26. J Dtsch Dermatol Ges. 2022. PMID: 35616215 Review.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Current uses of diagnostic high-frequency US in dermatology.Eur J Radiol. 1998 May;27 Suppl 2:S215-23. doi: 10.1016/s0720-048x(98)00065-5. Eur J Radiol. 1998. PMID: 9652525
Cited by
-
High-Frequency and Ultra-High-Frequency Ultrasound in Dermatologic Diseases and Aesthetic Medicine.Medicina (Kaunas). 2025 Jan 26;61(2):220. doi: 10.3390/medicina61020220. Medicina (Kaunas). 2025. PMID: 40005337 Free PMC article. Review.
References
-
- Crisan D., Wortsman X., Catalano O., Badea R., Kastler S., Badea A., Manea A., Scharffetter-Kochanek K., Strilciuc S., Crisan M., et al. Pre-operative high-frequency ultrasound: A reliable management tool in auricular and nasal non-melanoma skin cancer. J. Der Dtsch. Dermatol. Ges. 2024;22:357–365. doi: 10.1111/ddg.15308. - DOI - PubMed
-
- Wortsman X., Alfageme F., Roustan G., Arias-Santiago S., Martorell A., Catalano O., Scotto di Santolo M., Zarchi K., Bouer M., Gonzalez C., et al. Guidelines for Performing Dermatologic Ultrasound Examinations by the DERMUS Group. J. Ultrasound Med. 2016;35:577–580. doi: 10.7863/ultra.15.06046. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
