

Pre-Diagnosis Diet Predicts Response to Exclusive Enteral Nutrition and Correlates with Microbiome in Pediatric Crohn Disease
- PMID: 38613066
- PMCID: PMC11013084
- DOI: 10.3390/nu16071033
Pre-Diagnosis Diet Predicts Response to Exclusive Enteral Nutrition and Correlates with Microbiome in Pediatric Crohn Disease
Abstract
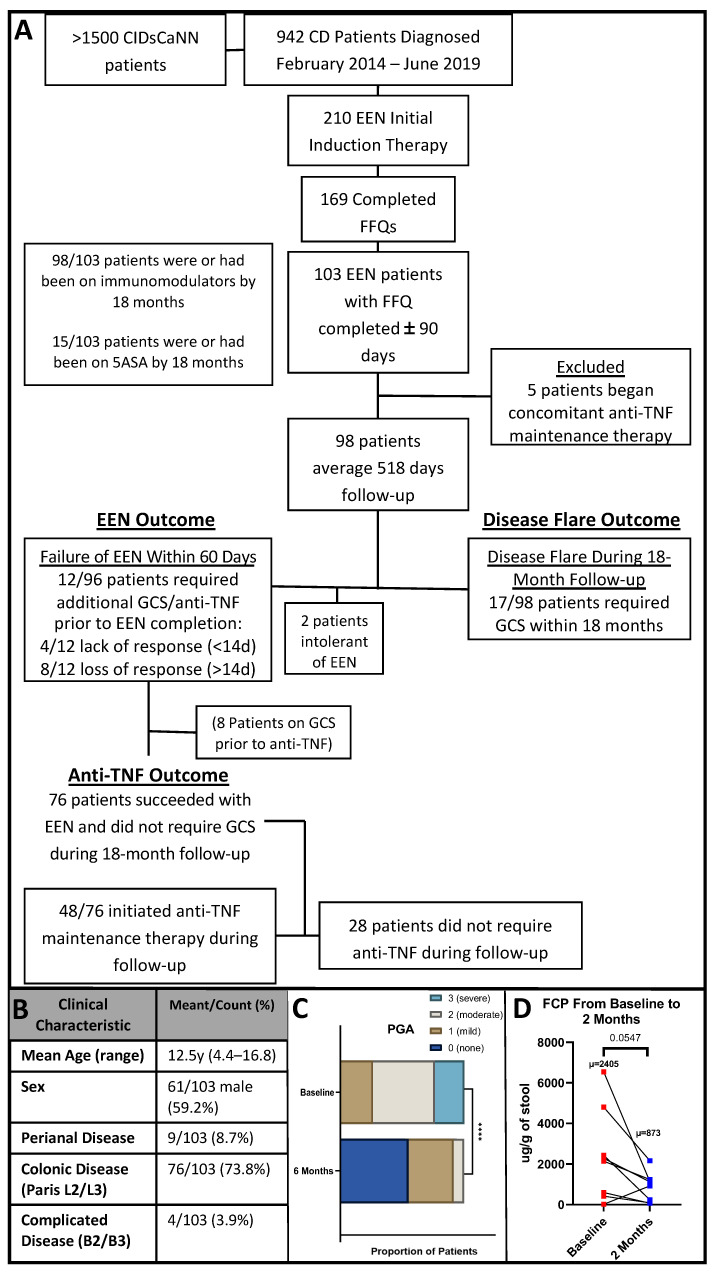
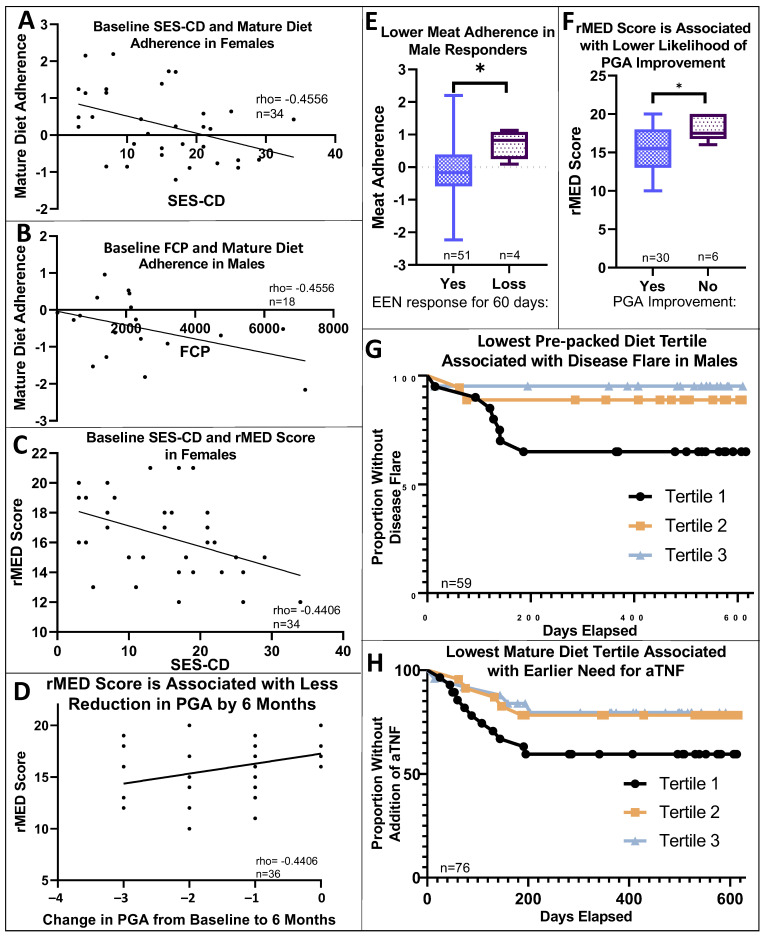
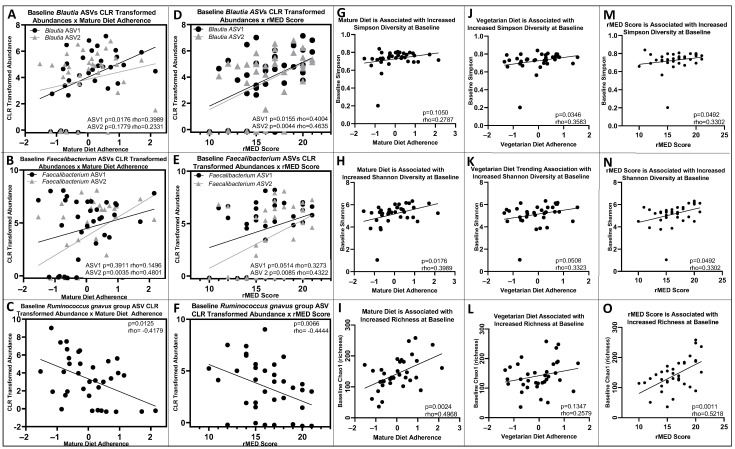
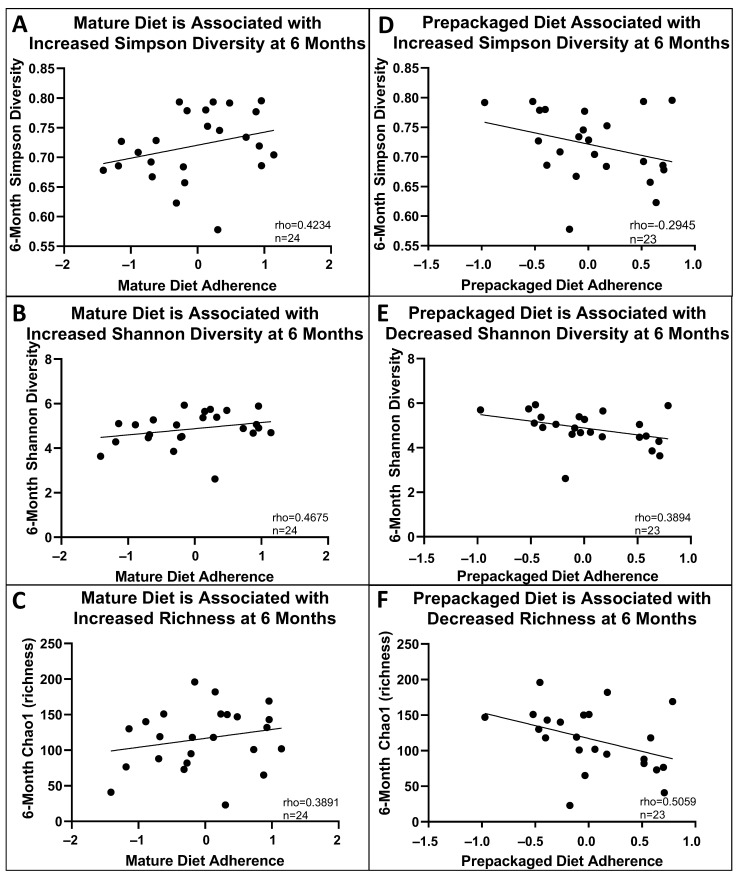
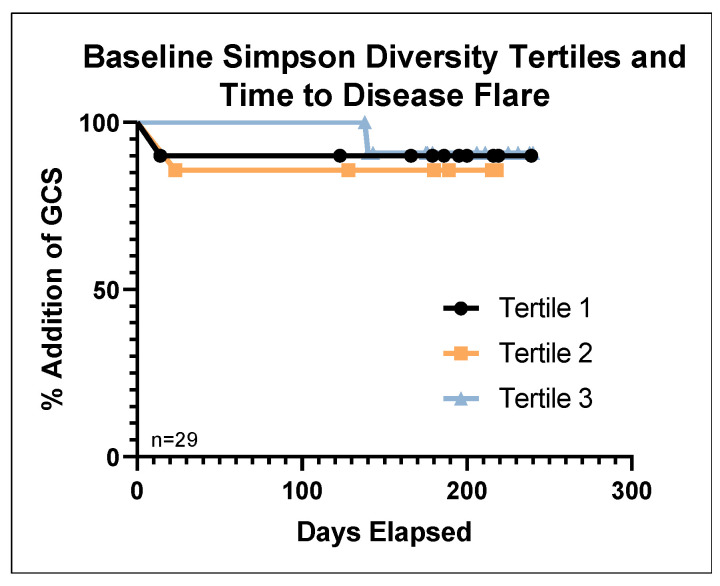
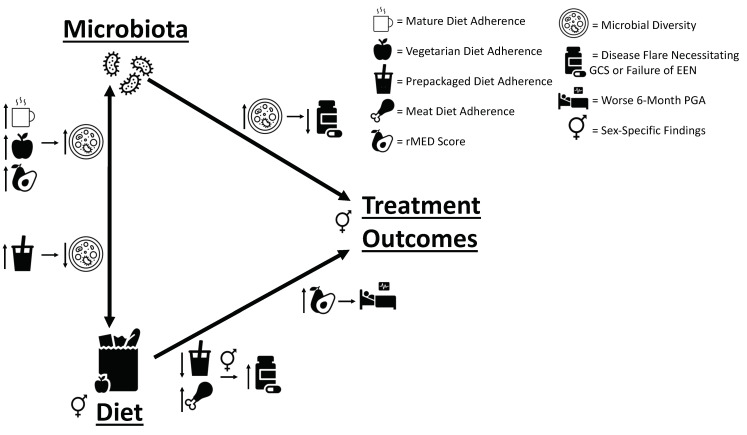
Exclusive enteral nutrition (EEN) is effective in inducing remission in pediatric Crohn disease (CD). EEN alters the intestinal microbiome, but precise mechanisms are unknown. We hypothesized that pre-diagnosis diet establishes a baseline gut microbiome, which then mediates response to EEN. We analyzed prospectively recorded food frequency questionnaires (FFQs) for pre-diagnosis dietary patterns. Fecal microbiota were sequenced (16SrRNA) at baseline and through an 18-month follow-up period. Dietary patterns, Mediterranean diet adherence, and stool microbiota were associated with EEN treatment outcomes, disease flare, need for anti-tumor necrosis factor (TNF)-α therapy, and long-term clinical outcomes. Ninety-eight patients were included. Baseline disease severity and microbiota were associated with diet. Four dietary patterns were identified by FFQs; a "mature diet" high in fruits, vegetables, and fish was linked to increased baseline microbial diversity, which was associated with fewer disease flares (p < 0.05) and a trend towards a delayed need for anti-TNF therapy (p = 0.086). Baseline stool microbial taxa were increased (Blautia and Faecalibacterium) or decreased (Ruminococcus gnavus group) with the mature diet compared to other diets. Surprisingly, a "pre-packaged" dietary pattern (rich in processed foods) was associated with delayed flares in males (p < 0.05). Long-term pre-diagnosis diet was associated with outcomes of EEN therapy in pediatric CD; diet-microbiota and microbiota-outcome associations may mediate this relationship.
Keywords: dietary pattern; inflammatory bowel diseases; microbiome; nutrition; pediatrics; prediction.
Conflict of interest statement
S.D., M.J., Z.Z., M.L., M.A., R.S., L.R., M.C., J.W., M.W.C., M.R., and M.G.S. have no conflicts to report. A.O. has served on an advisory board for AbbVie, Janssen, Pfizer, and Eli-Lilly; has received investigator-initiated research support from AbbVie; and has received educational grants from AbbVie and Janssen. M.S. has served as an advisory board member for AbbVie and is a speaker for Janssen and AbbVie. D.R.M. is a co-founder and shareholder of MedBiome Inc. K.J. has served as an advisory board member for AbbVie, Janssen, Amgen, Merck, Viatris, and McKesson Canada; is a member of AbbVie and Janssen Speaker’s bureau; and has received investigator-initiated research support from Janssen. J.C.d.B. served as an advisory board member and speaker for Abbvie, as well as an advisory board member for Janssen, Amgen, and Mylan. W.E.-M. served as an advisory board member and speaker’s panel member for AbbVie. C.D. served as an advisory board member and speaker for AbbVie, Organon, and Janssen. P.C.C. has received consulting fees from AbbVie, Janssen, Ferring, and Merck; honoraria from Abbvie and Amgen; investigator-initiated research support from AbbVie and Janssen; and educational grants from Janssen, Amgen, Takeda, and Viatris. Thomas D. Walters has received grants from AbbVie, Ferring; honoraria from AbbVie and Pfizer; and served as an advisory board member for AbbVie, Janssen, and Pfizer. H.Q.H. served as an advisory board member and speaker for AbbVie. A.M.G. reports consulting fees from AbbVie, Amgen, BristolMyersSquibb, Janssen, Lilly, Merck, and Pfizer; speaker fees from AbbVie, Janssen, and Nestle; and investigator-initiated research support from AbbVie. E.W. reports personal fees from AbbVie, Janssen, Nestle Health Sciences, BioJamp, Pfizer, and Mead Johnson Nutrition. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Kuenzig M.E., Fung S.G., Marderfeld L., Mak J.W.Y., Kaplan G.G., Ng S.C., Wilson D.C., Cameron F., Henderson P., Kotze P.G., et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: Systematic Review. Gastroenterology. 2022;162:1147–1159.e4. doi: 10.1053/j.gastro.2021.12.282. - DOI - PubMed
-
- Dijk S., Armstrong H., Valcheva R., Wine E. Paediatric IBD: The host, diet & microbes in pathogenesis & treatment: A narrative review. Dig. Med. Res. 2021;4 doi: 10.21037/dmr-20-160. - DOI
-
- Johnson A.J., Vangay P., Al-Ghalith G.A., Hillmann B.M., Ward T.L., Shields-Cutler R.R., Kim A.D., Shmagel A.K., Syed A.N., Students P.M.C. Daily sampling reveals personalized diet-microbiome associations in humans. Cell Host Microbe. 2019;25:789–802.e5. doi: 10.1016/j.chom.2019.05.005. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
