

Toward clinical exomes in diagnostics and management of male infertility
- PMID: 38614076
- PMCID: PMC11080280
- DOI: 10.1016/j.ajhg.2024.03.013
Toward clinical exomes in diagnostics and management of male infertility
Abstract
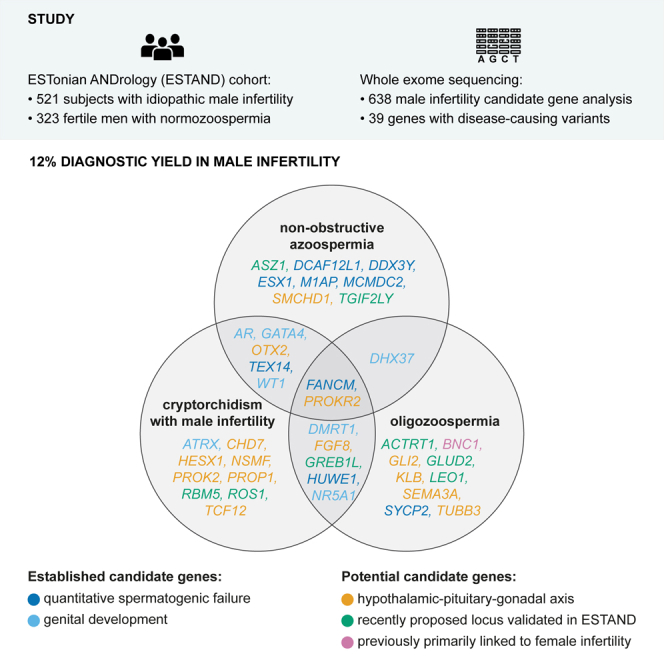
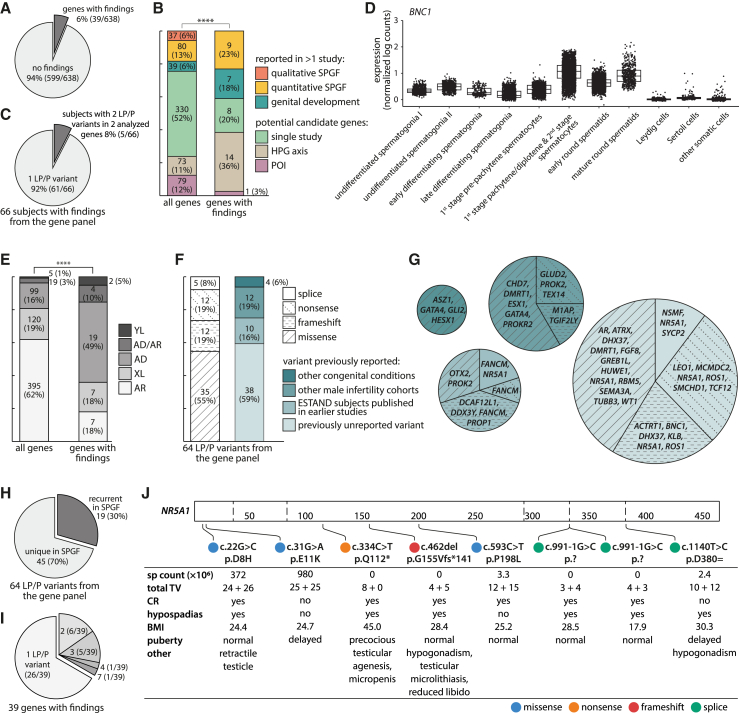
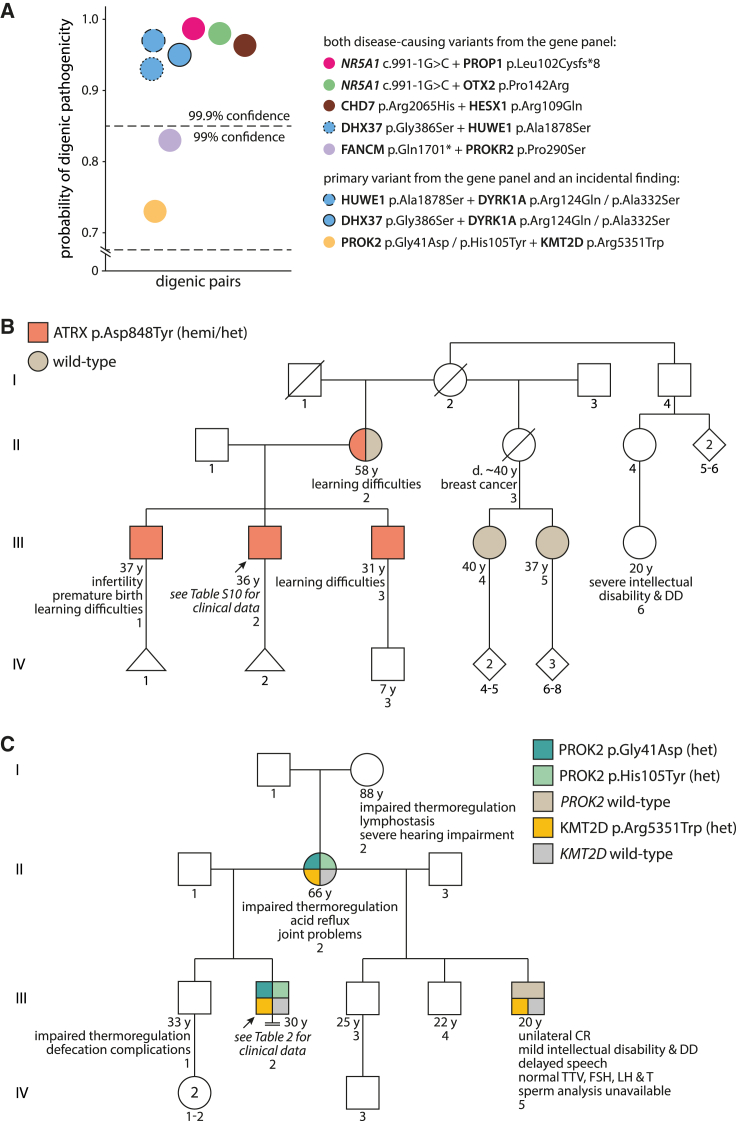
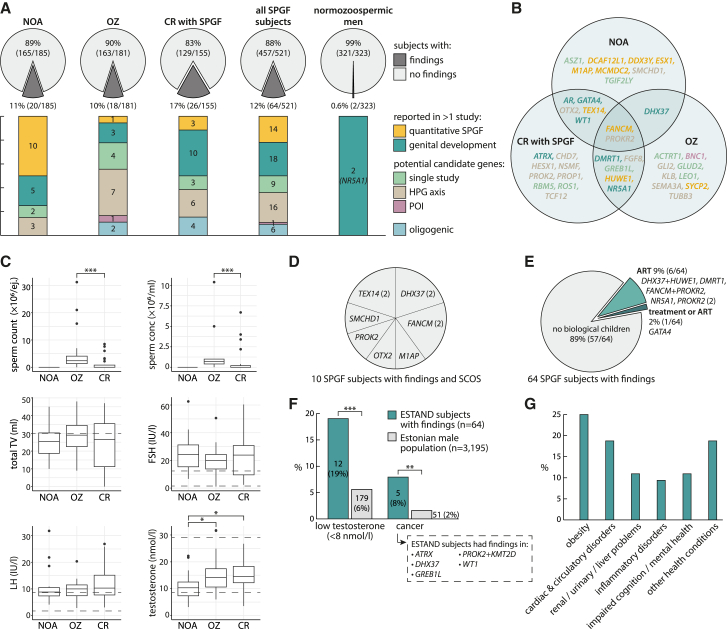
Infertility, affecting ∼10% of men, is predominantly caused by primary spermatogenic failure (SPGF). We screened likely pathogenic and pathogenic (LP/P) variants in 638 candidate genes for male infertility in 521 individuals presenting idiopathic SPGF and 323 normozoospermic men in the ESTAND cohort. Molecular diagnosis was reached for 64 men with SPGF (12%), with findings in 39 genes (6%). The yield did not differ significantly between the subgroups with azoospermia (20/185, 11%), oligozoospermia (18/181, 10%), and primary cryptorchidism with SPGF (26/155, 17%). Notably, 19 of 64 LP/P variants (30%) identified in 28 subjects represented recurrent findings in this study and/or with other male infertility cohorts. NR5A1 was the most frequently affected gene, with seven LP/P variants in six SPGF-affected men and two normozoospermic men. The link to SPGF was validated for recently proposed candidate genes ACTRT1, ASZ1, GLUD2, GREB1L, LEO1, RBM5, ROS1, and TGIF2LY. Heterozygous truncating variants in BNC1, reported in female infertility, emerged as plausible causes of severe oligozoospermia. Data suggested that several infertile men may present congenital conditions with less pronounced or pleiotropic phenotypes affecting the development and function of the reproductive system. Genes regulating the hypothalamic-pituitary-gonadal axis were affected in >30% of subjects with LP/P variants. Six individuals had more than one LP/P variant, including five with two findings from the gene panel. A 4-fold increased prevalence of cancer was observed in men with genetic infertility compared to the general male population (8% vs. 2%; p = 4.4 × 10-3). Expanding genetic testing in andrology will contribute to the multidisciplinary management of SPGF.
Keywords: monogenic infertility, azoospermia, oligozoospermia, cryptorchidism, exome sequencing, gene panel, molecular diagnostics, diagnostic yield, oligogenic, infertility management.
Copyright © 2024 American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Chen S., Wang G., Zheng X., Ge S., Dai Y., Ping P., Chen X., Liu G., Zhang J., Yang Y., et al. Whole-exome sequencing of a large Chinese azoospermia and severe oligospermia cohort identifies novel infertility causative variants and genes. Hum. Mol. Genet. 2020;29:2451–2459. doi: 10.1093/HMG/DDAA101. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
