

Host-microbiome associations in saliva predict COVID-19 severity
- PMID: 38617584
- PMCID: PMC11010653
- DOI: 10.1093/pnasnexus/pgae126
Host-microbiome associations in saliva predict COVID-19 severity
Abstract
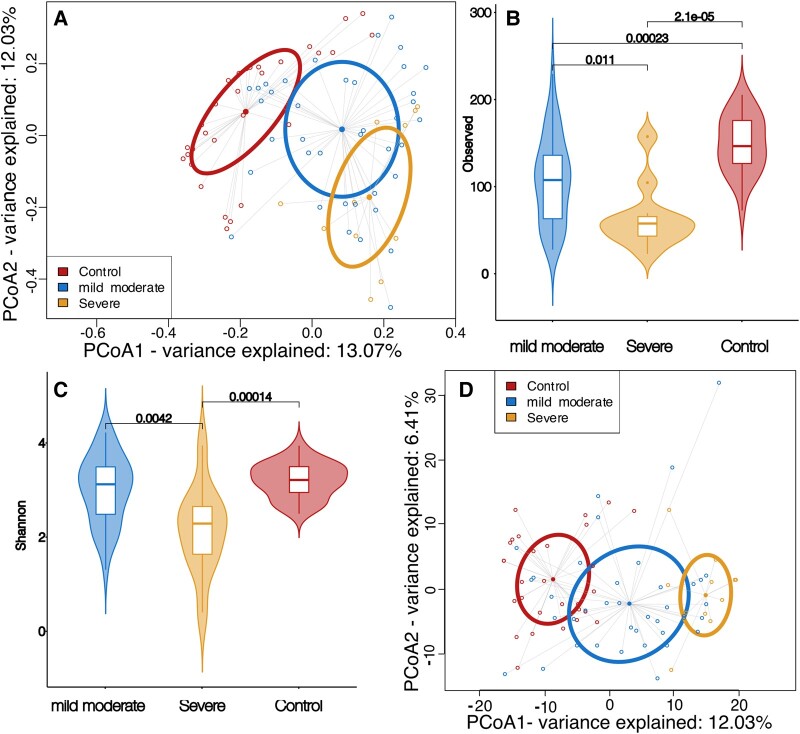
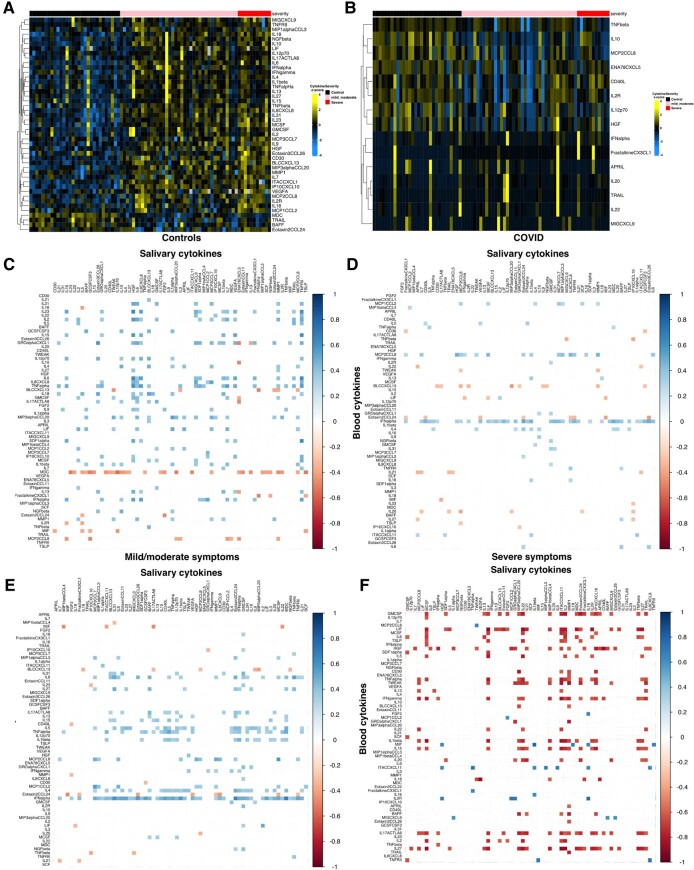
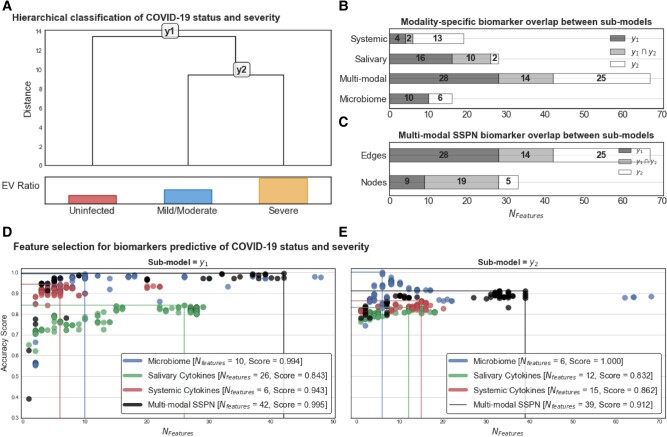
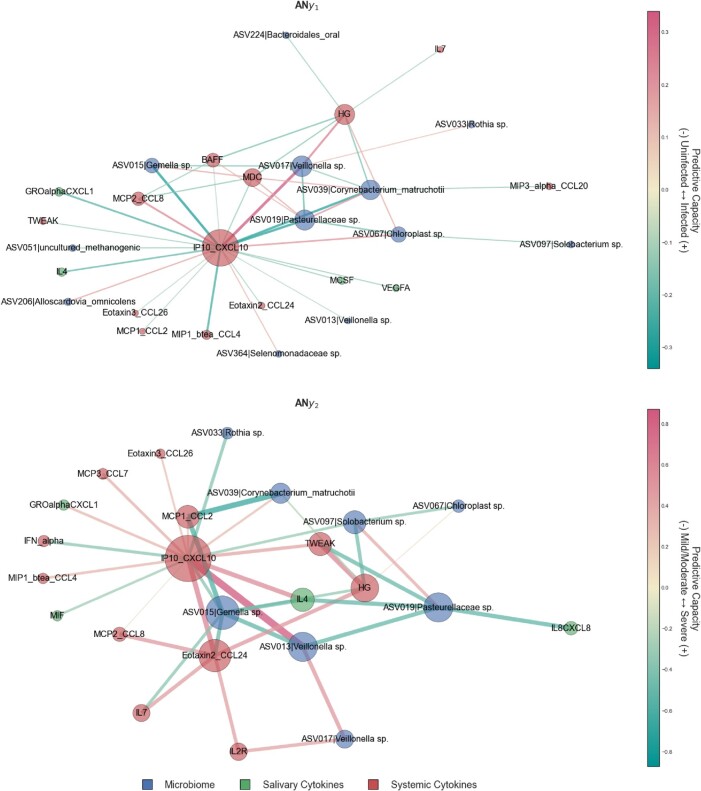
Established evidence indicates that oral microbiota plays a crucial role in modulating host immune responses to viral infection. Following severe acute respiratory syndrome coronavirus 2, there are coordinated microbiome and inflammatory responses within the mucosal and systemic compartments that are unknown. The specific roles the oral microbiota and inflammatory cytokines play in the pathogenesis of coronavirus disease 2019 (COVID-19) are yet to be explored. Here, we evaluated the relationships between the salivary microbiome and host parameters in different groups of COVID-19 severity based on their oxygen requirement. Saliva and blood samples (n = 80) were collected from COVID-19 and from noninfected individuals. We characterized the oral microbiomes using 16S ribosomal RNA gene sequencing and evaluated saliva and serum cytokines and chemokines using multiplex analysis. Alpha diversity of the salivary microbial community was negatively associated with COVID-19 severity, while diversity increased with health. Integrated cytokine evaluations of saliva and serum showed that the oral host response was distinct from the systemic response. The hierarchical classification of COVID-19 status and respiratory severity using multiple modalities separately (i.e. microbiome, salivary cytokines, and systemic cytokines) and simultaneously (i.e. multimodal perturbation analyses) revealed that the microbiome perturbation analysis was the most informative for predicting COVID-19 status and severity, followed by the multimodal. Our findings suggest that oral microbiome and salivary cytokines may be predictive of COVID-19 status and severity, whereas atypical local mucosal immune suppression and systemic hyperinflammation provide new cues to understand the pathogenesis in immunologically compromised populations.
Keywords: COVID-19; host-microbial; inflammatory cytokines; machine learning; saliva microbiome.
© The Author(s) 2024. Published by Oxford University Press on behalf of National Academy of Sciences.
Figures
Update of
-
Host-Microbiome Associations in Saliva Predict COVID-19 Severity.bioRxiv [Preprint]. 2023 May 3:2023.05.02.539155. doi: 10.1101/2023.05.02.539155. bioRxiv. 2023. Update in: PNAS Nexus. 2024 Mar 25;3(4):pgae126. doi: 10.1093/pnasnexus/pgae126. PMID: 37205528 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
