

Leveraging multi-tier healthcare facility network simulations for capacity planning in a pandemic
- PMID: 38620120
- PMCID: PMC10290165
- DOI: 10.1016/j.seps.2023.101660
Leveraging multi-tier healthcare facility network simulations for capacity planning in a pandemic
Abstract
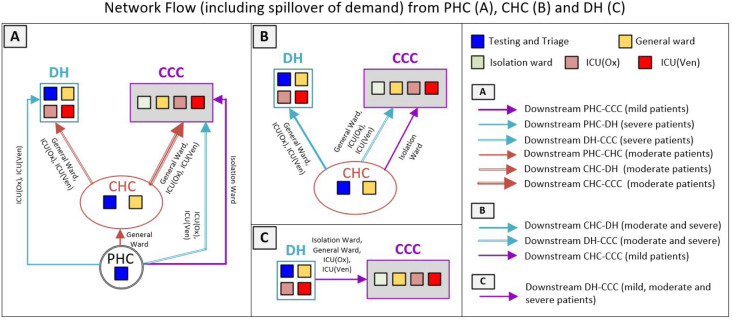
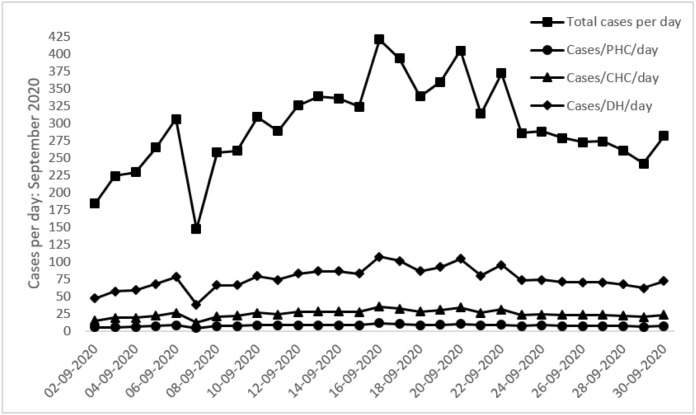
The COVID-19 pandemic has placed severe demands on healthcare facilities across the world, and in several countries, makeshift COVID-19 centres have been operationalised to handle patient overflow. In developing countries such as India, the public healthcare system (PHS) is organised as a hierarchical network with patient flows from lower-tier primary health centres (PHC) to mid-tier community health centres (CHC) and downstream to district hospitals (DH). In this study, we demonstrate how a network-based modelling and simulation approach utilising generic modelling principles can (a) quantify the extent to which the existing facilities in the PHS can effectively cope with the forecasted COVID-19 caseload; and (b) inform decisions on capacity at makeshift COVID-19 Care Centres (CCC) to handle patient overflows. We apply the approach to an empirical study of a local PHS comprising ten PHCs, three CHCs, one DH and one makeshift CCC. Our work demonstrates how the generic modelling approach finds extensive use in the development of simulations of multi-tier facility networks that may contain multiple instances of generic simulation models of facilities at each network tier. Further, our work demonstrates how multi-tier healthcare facility network simulations can be leveraged for capacity planning in health crises.
Keywords: COVID-19 operations; Capacity planning; Healthcare network simulation; OR in developing countries.
© 2023 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Structural capacity and continuum of snakebite care in the primary health care system in India: a cross-sectional assessment.BMC Prim Care. 2023 Aug 11;24(1):160. doi: 10.1186/s12875-023-02109-2. BMC Prim Care. 2023. PMID: 37563556 Free PMC article.
-
A model for national assessment of barriers for implementing digital technology interventions to improve hypertension management in the public health care system in India.BMC Health Serv Res. 2021 Oct 15;21(1):1101. doi: 10.1186/s12913-021-06999-9. BMC Health Serv Res. 2021. PMID: 34654431 Free PMC article.
-
Primary Health Care Facility Preparedness for Outpatient Service Provision During the COVID-19 Pandemic in India: Cross-Sectional Study.JMIR Public Health Surveill. 2020 Jun 1;6(2):e19927. doi: 10.2196/19927. JMIR Public Health Surveill. 2020. PMID: 32452819 Free PMC article.
-
Harnessing the potential of the primary healthcare facilities in India to respond COVID-19 pandemic: A scoping evidence-based research synthesis.J Family Med Prim Care. 2021 Jan;10(1):116-121. doi: 10.4103/jfmpc.jfmpc_1609_20. Epub 2021 Jan 30. J Family Med Prim Care. 2021. PMID: 34017712 Free PMC article. Review.
-
Travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2020 Oct 5;10:CD013717. doi: 10.1002/14651858.CD013717. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 25;3:CD013717. doi: 10.1002/14651858.CD013717.pub2. PMID: 33502002 Updated.
Cited by
-
Improving the usability of open health service delivery simulation models using Python and web apps.NIHR Open Res. 2023 Dec 15;3:48. doi: 10.3310/nihropenres.13467.2. eCollection 2023. NIHR Open Res. 2023. PMID: 37881450 Free PMC article.
References
-
- Leite H., Lindsay C., Kumar M. COVID-19 outbreak: Implications on healthcare operations. TQM J. 2020;33(1):247–256. doi: 10.1108/TQM-05-2020-0111. - DOI
-
- Roy S.N., Shah B.J., Gajjar H. Application of simulation in healthcare service operations: A review and research agenda. ACM Trans Model Comput Simul. 2020;31(1):1–23.
-
- Mustafee N., Katsaliaki K. Classification of the existing knowledge base of OR/MS research and practice (1990–2019) using a proposed classification scheme. Comput Oper Res. 2020;118:1–17. doi: 10.1016/j.cor.2020.104920. - DOI
-
- Garcia-Vicuña D., Mallor F., Esparza L. In: Proceedings of the 2020 winter simulation conference. Bae K.-H., Feng B., Kim S., Lazarova-Molnar S., Zheng Z., Roeder T., Thiesing R., editors. Institute of Electrical and Electronics Engineers, Inc.; Piscataway, New Jersey: 2020. Planning ward and intensive care unit beds for COVID-19 patients using a discrete event simulation model; pp. 759–770.
LinkOut - more resources
Full Text Sources