

Review
doi: 10.1016/j.yacr.2021.04.010.
Epub 2021 Jun 2.
Emerging Pulmonary Infections in Clinical Practice
Affiliations
- PMID: 38620910
- PMCID: PMC8169325
- DOI: 10.1016/j.yacr.2021.04.010
Item in Clipboard
Review
Emerging Pulmonary Infections in Clinical Practice
Adv Clin Radiol.
2021 Sep.
No abstract available
Keywords: Computed tomography; Emerging infections; Pulmonary infection.
Figures
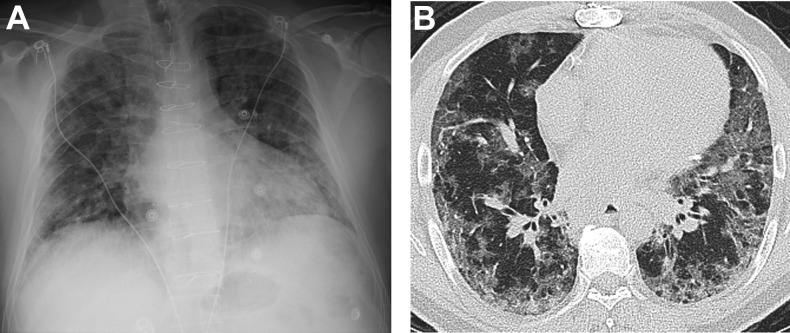
Acute typical appearance of COVID-19 in a 50-year-old man. Frontal chest radiograph (A) shows bilateral perihilar and peripheral hazy airspace opacities without pleural effusions. Axial chest CT (B) demonstrates bilateral peribronchovascular and peripheral ground glass opacities.
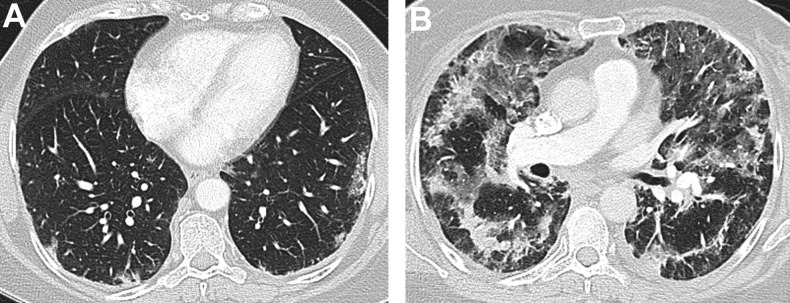
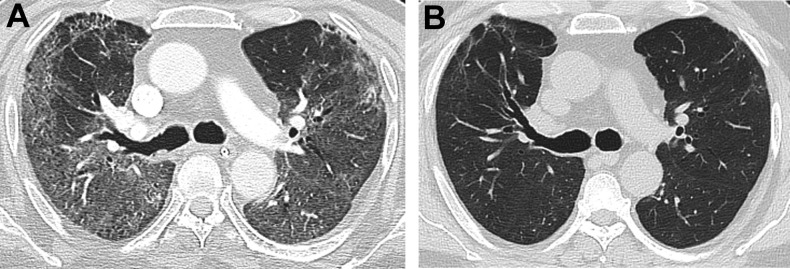
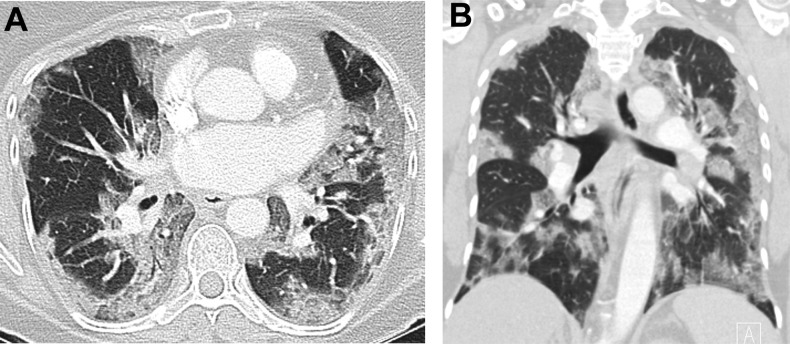
Progression of COVID-19 in a 60-year-old woman. Axial chest CT on initial presentation (A) with very mild peripheral ground glass opacities. Axial chest CT obtained 3 weeks later (B) now shows extensive bilateral peribronchovascular and peripheral ground glass opacities and consolidation, with areas of subpleural sparing and perilobular pattern similar to organizing pneumonia.

Reverse halo in a 62-year-old man with COVID-19. Axial chest CT shows an area in the anterior right middle lobe of central low attenuation and peripheral high attenuation, the “reverse halo,” or “Atoll,” sign. Extensive bilateral ground glass and focal consolidative opacities in a peripheral and peribronchovascular pattern, as well as perilobular pattern, are also seen.
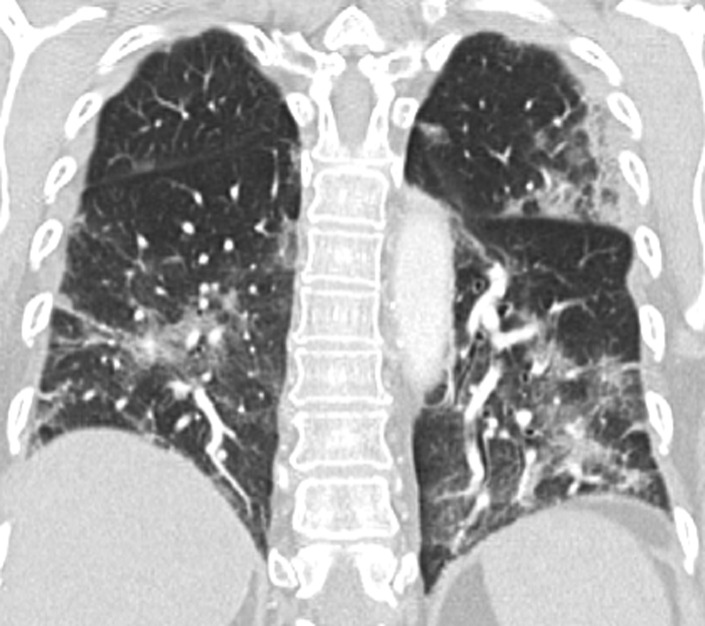
Vessel dilation in a 62-year-old woman. Coronal chest CT demonstrates dilated pulmonary arteries that reach the lung periphery. Bilateral peripheral and peribronchovascular ground glass opacities are also present.

Barotrauma in a 68-year-old man with COVID-19. Axial chest CT demonstrates extensive pneumomediastinum. Bilateral peribronchovascular and peripheral ground glass opacities, consolidation, and bronchiectasis are seen, compatible with the patient’s COVID-19 infection.
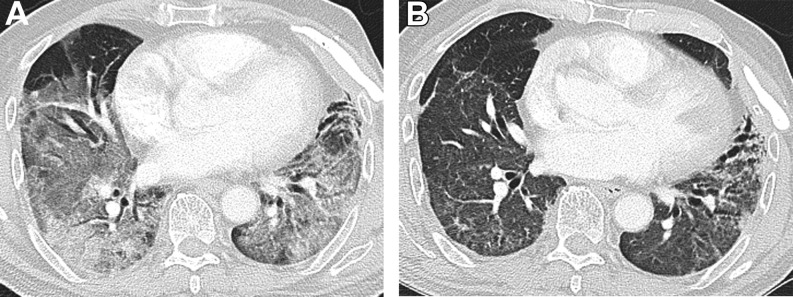
Convalescent COVID-19 in a 71-year-old man. Axial chest CT from initial hospitalization (A) shows extensive bilateral ground glass opacities and mild bronchiectasis in the lingula. (B) Follow-up CT performed 4 months later demonstrates significant improvement in the ground glass opacities, but with increased bronchiectasis in the lingula and left-greater-than-right lower lobes.
Convalescent COVID-19 in a 62-year-old man. Axial chest CT images from initial hospitalization (A) demonstrate bilateral peribronchovascular and peripheral ground glass opacities with areas of perilobular pattern. Mild traction bronchiectasis is also seen in the anterior upper and lower lobes. Follow-up CT image performed 9 months later (B) shows essential resolution of the ground glass opacities, with mild residual perilobular pattern. The bronchiectasis has also improved overall.
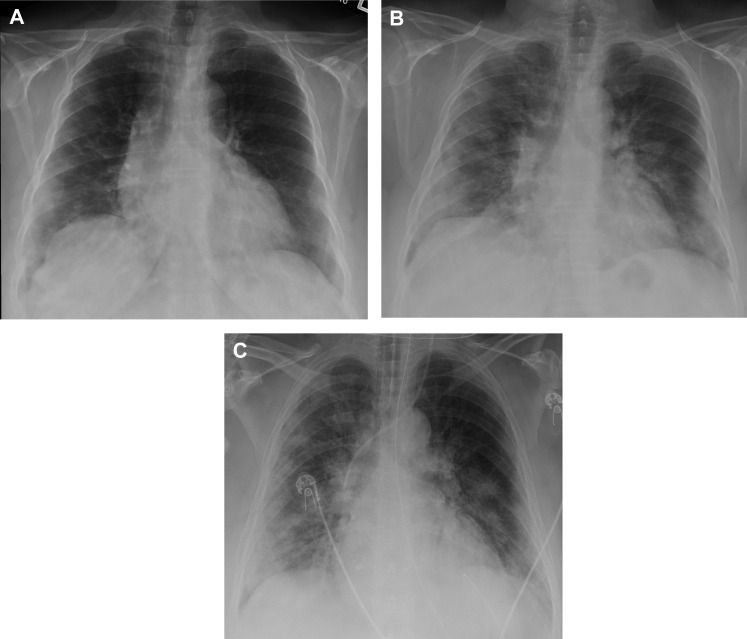
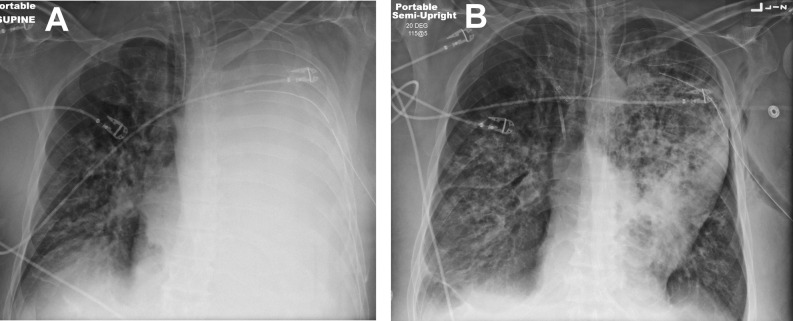
. Progression of H1N1 influenza in a 58-year-old woman. Initial frontal chest radiograph (A) demonstrates mild bilateral, right-greater-than-left peripheral hazy airspace opacities. Chest radiographs obtained 2 (B) and 3 (C) days later demonstrate increasing bilateral hazy airspace opacities with progressive perihilar involvement.
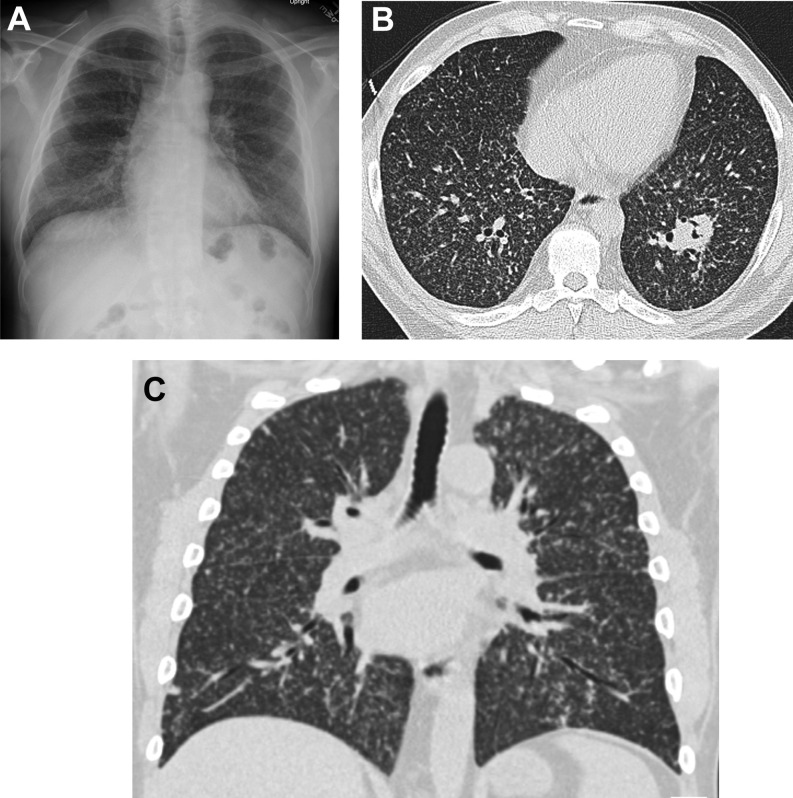
Forty-four-year-old man with H1N1 influenza. Frontal chest radiograph (A) shows bilateral perihilar and peripheral hazy opacities. On axial chest CT (B), there are peripheral and peribronchovascular ground glass opacities and consolidation.
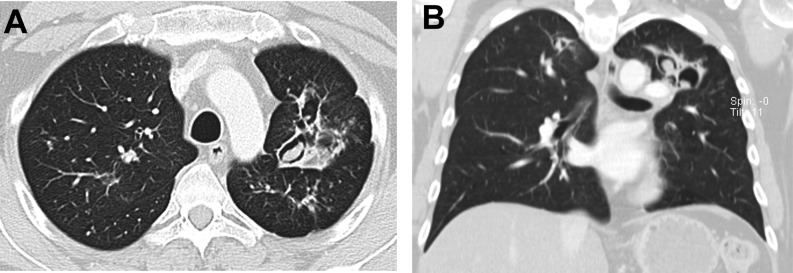
Sixty-six-year-old man with H1N3 influenza. Axial chest CT images (A, B) show bilateral peribronchovascular ground glass opacities in a pattern similar to organizing pneumonia. Bronchial wall thickening is also apparent in the lower lobes (B).
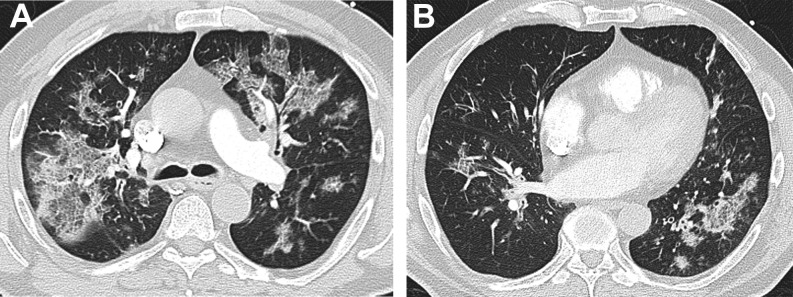
Fifty-two-year-old woman with H1N1 influenza. Axial (A) and coronal (B) CT images show peripheral and peribronchovascular ground glass opacities in a pattern similar to organizing pneumonia.
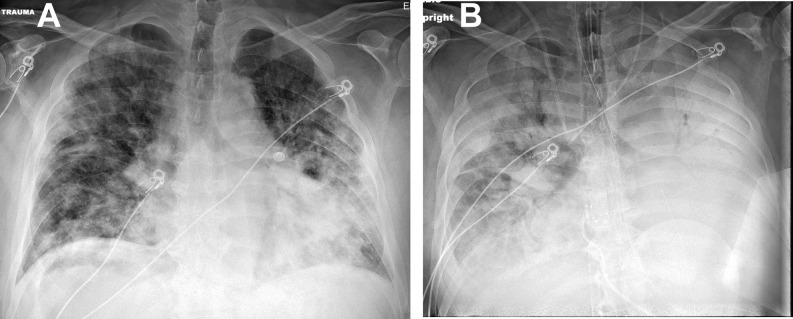
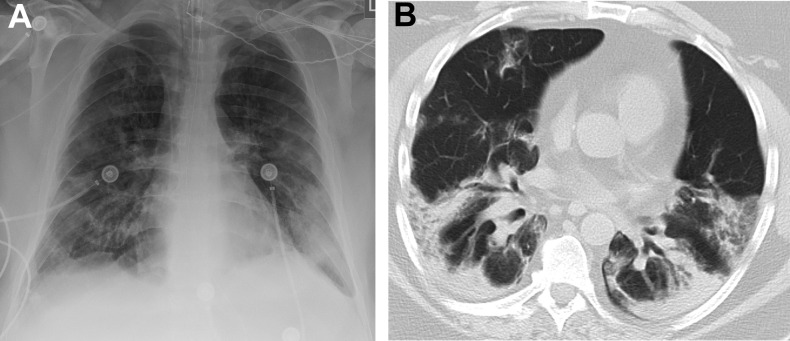
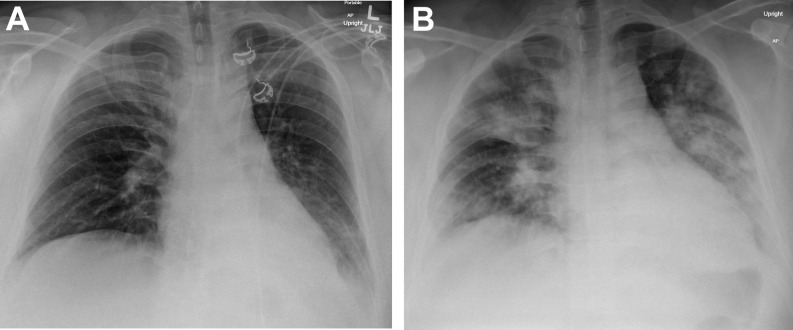
Superinfection of HMPV with legionella. Frontal chest radiograph in a 71-year-old man (A) on presentation shows bilateral ground glass opacities. Chest radiograph on day 2 (B) shows rapid progression with complete opacification of the left lung and extensive ground glass opacities and consolidation in the right lung.
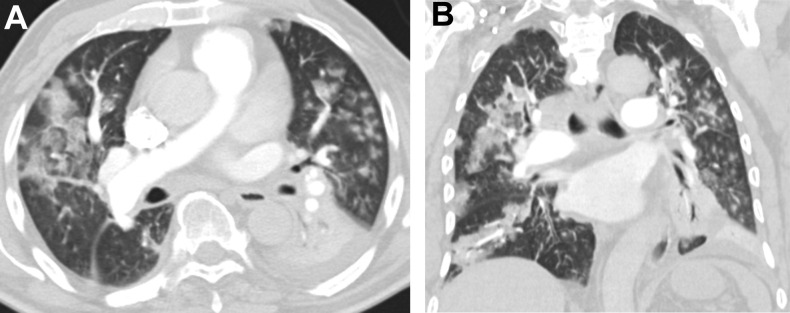
Sixty-three-year-old man with human metapneumovirus (HPMV). Axial (A) and coronal (B) chest CTs show bilateral peribronchovascular ground glass opacities, centrilobular nodules, and left lower lobe consolidation.
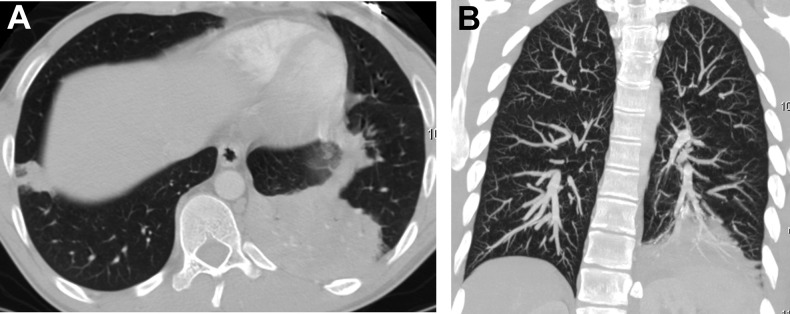
Adenovirus pneumonia in a 40-year-old man. Axial (A) and coronal maximum intensity projection (MIP) (B) chest CT images show right lower lobe consolidation. The MIP images underscore the absence of centrilobular nodules.
Progression of legionella in a 33-year-old man. Initial chest radiograph (A) demonstrates a left retrocardiac consolidation. Chest radiograph obtained 3 days later (B) shows marked progression with new multifocal bilateral consolidation.
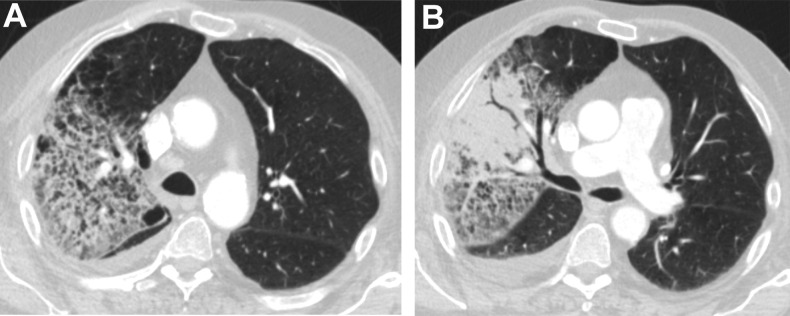
Legionella in a 68-year-old man with underlying emphysema. Axial chest CTs (A, B) demonstrate right upper lobe ground glass opacities, consolidation, and a small right pleural effusion, with an absence of centrilobular nodules. There is a background of centrilobular emphysema.
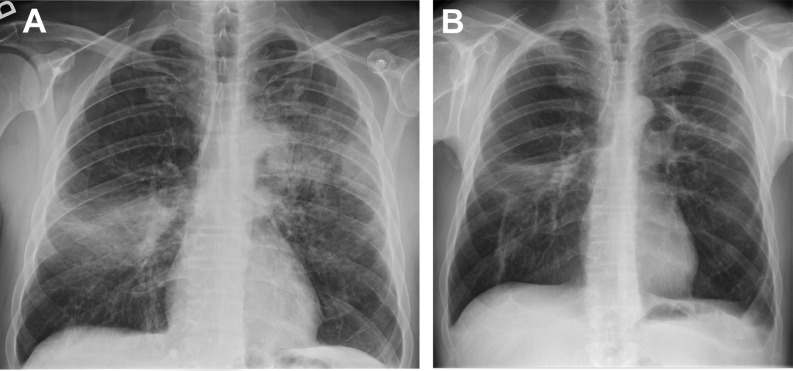
Legionella in a 53-year-old man. Initial chest radiograph (A) demonstrates left upper lung and right mid lung consolidation. Follow-up radiograph 3 months after treatment (B) shows persistent opacities, with bandlike consolidation in the left upper lung and more organized, contracted consolidation in the right mid lung. These opacities may represent organizing pneumonia.
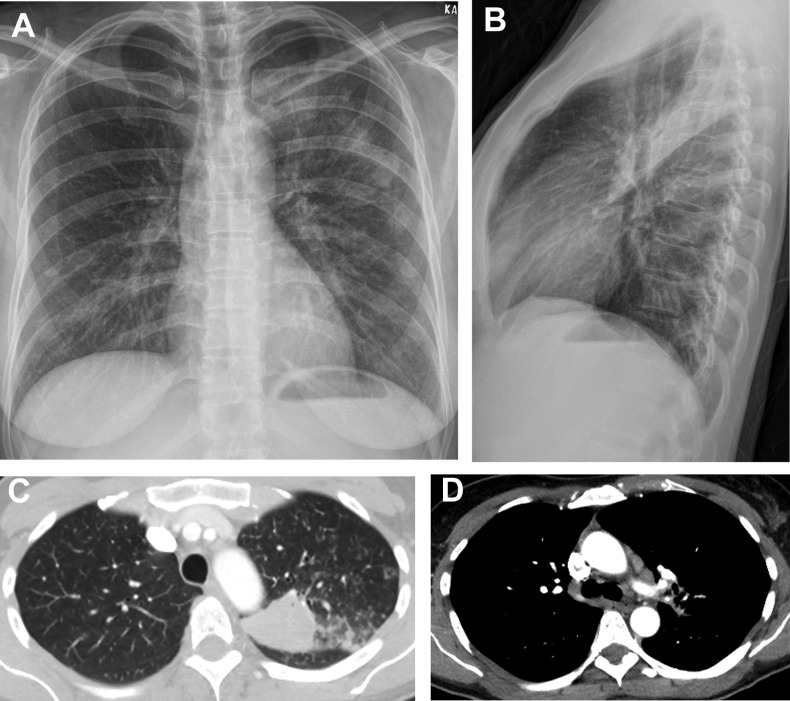
Fifty-two-year-old woman with recent travel to California, presenting with fever and cough, found to have coccidioidomycosis. Posteroanterior and lateral chest radiographs and chest CT (A–C) show left upper lobe consolidation with a similar appearance as bacterial community-acquired pneumonia. Enlarged left mediastinal lymph nodes are also present (D).
Sixty-year-old man with coccidioidomycosis and empyema. Initial frontal chest radiograph (A) demonstrates a large left pleural effusion. A chest tube was placed (B), and residual bilateral consolidation and nodular opacities are present.
Disseminated coccidioidomycosis in a 46-year-old man with prior renal transplant. Frontal chest radiograph (A), axial chest CT (B), and coronal chest CT (C) show innumerable bilateral randomly distributed miliary nodules. Focal left upper lobe consolidation is also demonstrated on CT (B).
Thin-walled cavity of chronic coccidioidomycosis in a 42-year-old-woman. Posteroanterior chest radiograph (A) and coronal CT (B) demonstrate left upper lobe thin-walled cavity with adjacent bronchiectasis and pleural thickening.
Thin-walled cavity of chronic coccidioidomycosis with mycetoma in a 31-year-old man. Axial (A) and coronal (B) chest CT show left upper lobe thin-walled cavity with internal circumscribed nodules with smooth borders compatible with mycetoma.
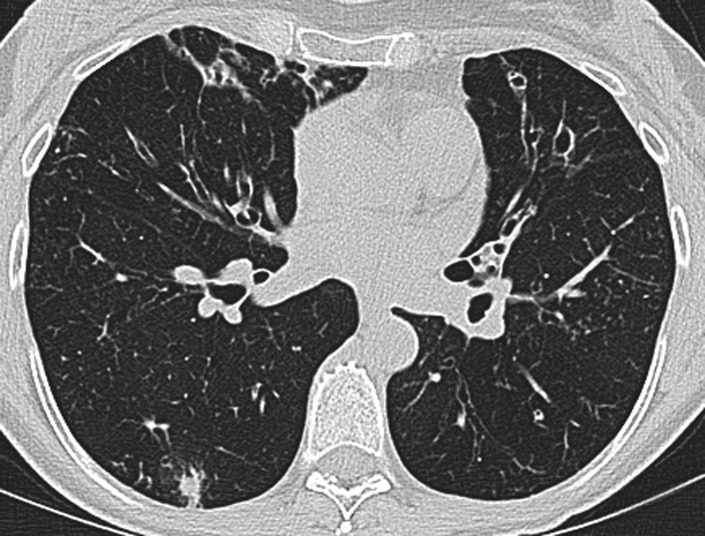
Typical appearance of MAC. Axial chest CT in a 64-year-old woman demonstrates multifocal areas of cylindrical bronchiectasis, especially in the right middle lobe and lingula, with tree-in-bud centrilobular nodules and at least one larger discrete nodule.
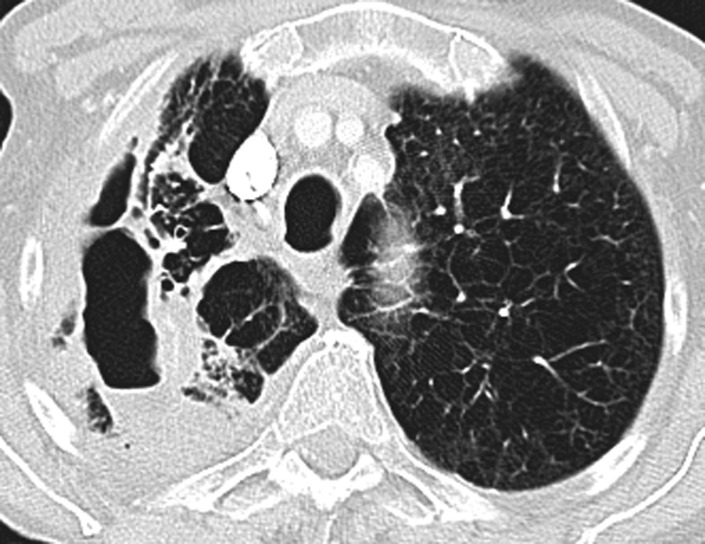
Severe cavitary MAC in a 58-year-old man with emphysema. Axial chest CT shows a large, thick-walled right upper lobe cavity with adjacent consolidation and internal air-fluid level.
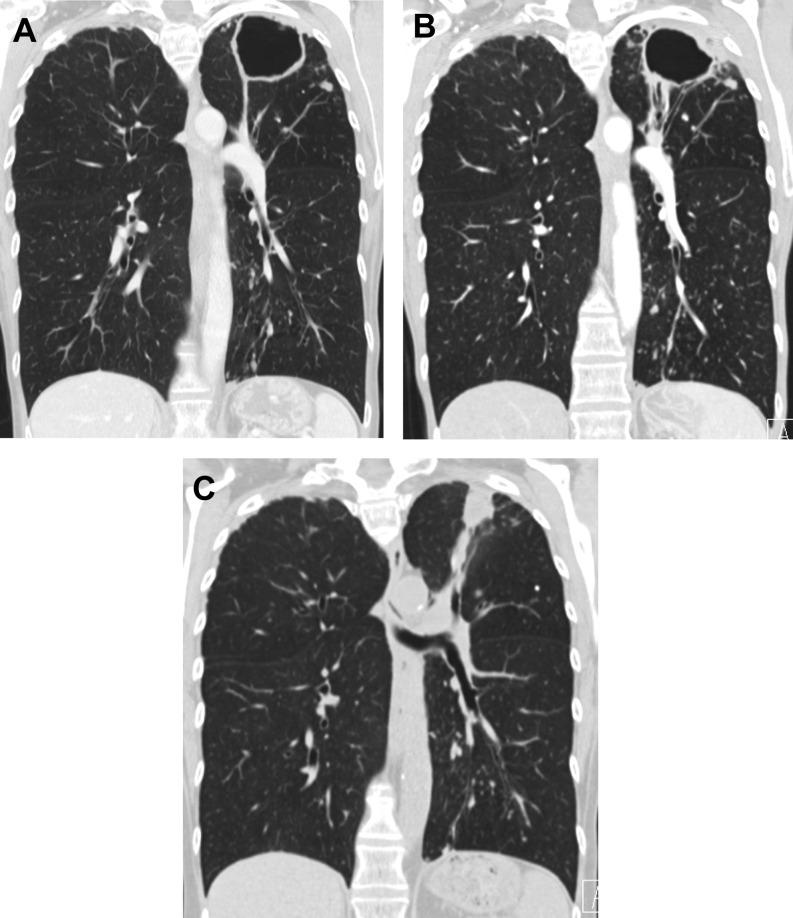
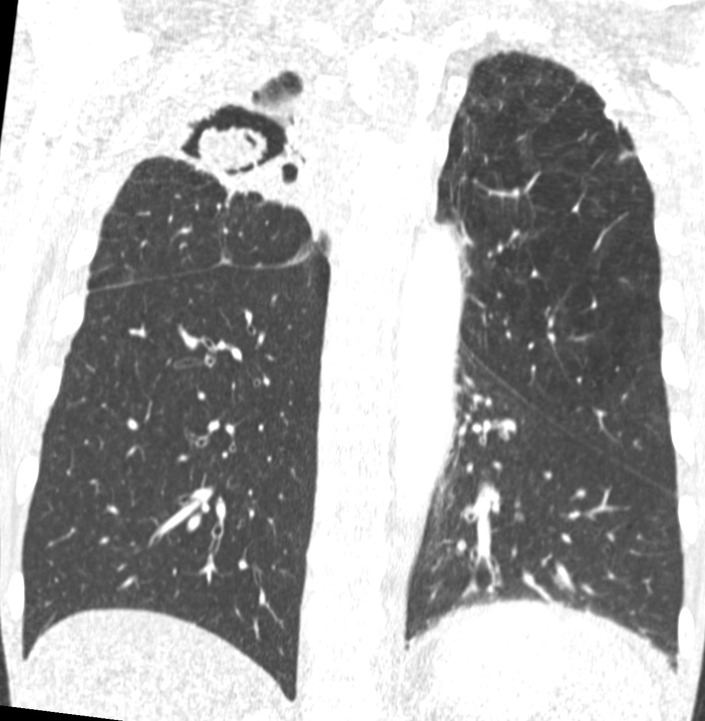
Thin-walled cavitary MAC in a 56-year-old woman. Coronal chest CTs before treatment (A, B) show a thin-walled cavity that develops adjacent pleural thickening and nodularity. Coronal chest CT following treatment (C) shows collapse of the cavity with residual nodule.
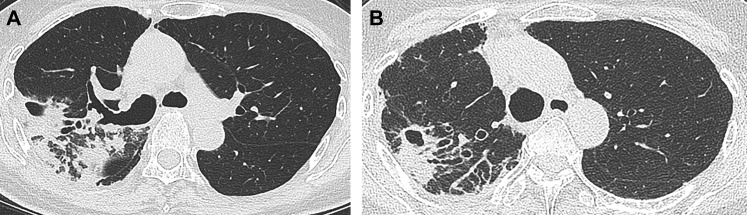
Mycobacterium abscessus in a 50-year-old man. Axial chest CT (A) demonstrates largely thick-walled cavity and nearby bronchiectasis. Follow-up chest CT 4 years later (B) shows improvement in cavity size, but with increased bronchiectasis.
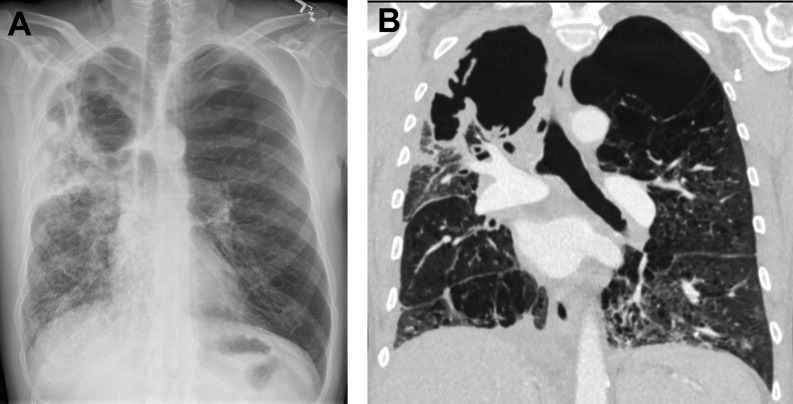
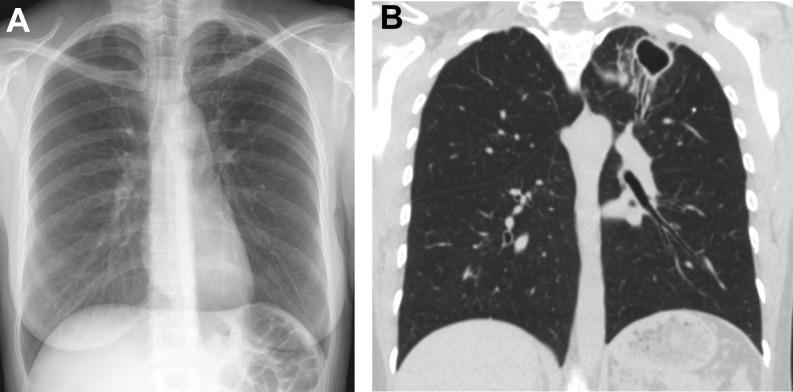
Chronic cavitary aspergillosis in a 62-year-old man with emphysema. Chest radiograph (A) and coronal chest CT (B) show an irregular relatively thick-walled cavity with adjacent pleural thickening. Nodules can also be seen in the right lower lung (A) and left lower lung (B).
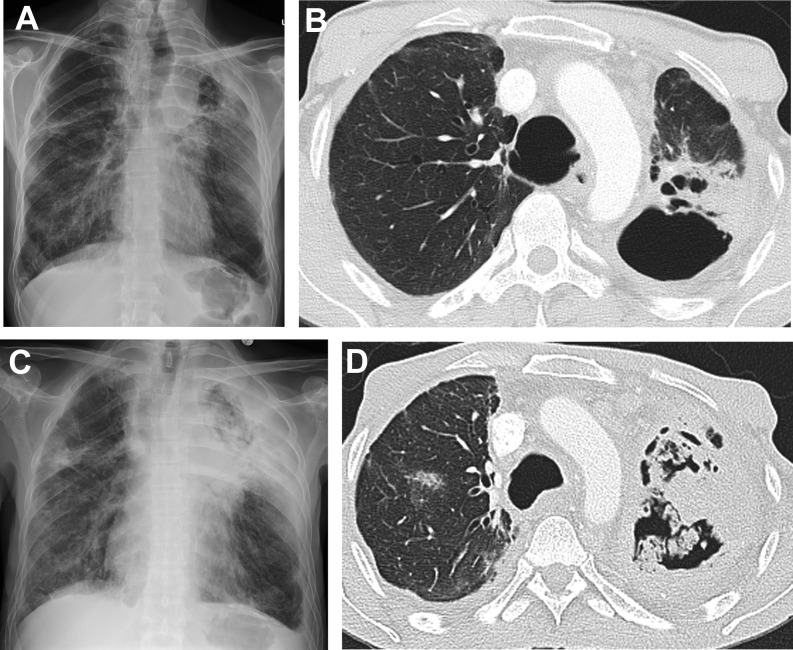
Progression of chronic aspergillosis in a 49-year-old man with underlying emphysema. Chest radiograph (A) and axial chest CT (B) show thick-walled left upper lobe cavity with adjacent consolidation. Several months later, chest radiograph (C) and chest CT (D) show marked increase in cavity wall thickness, internal aspergilloma formation, and adjacent pleural thickening.
Chronic aspergillosis superimposed on nontuberculous mycobacterial infection in a 57-year-old man. Extensive pleural thickening is present adjacent to the right upper lobe cavity, and an aspergilloma is also conspicuous.
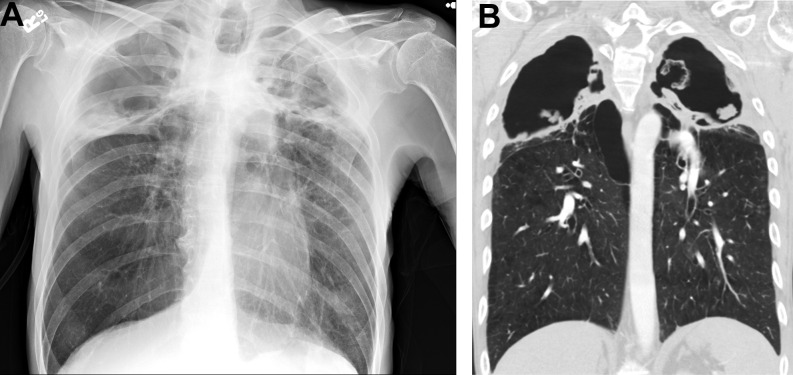
Aspergilloma in a 65-year-old man. Frontal chest radiograph (A) and coronal chest CT (B) show bilateral thick-walled apical cavities with internal debris including an organized aspergilloma on the left.
Similar articles
-
The role of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (FDG PET/CT) in assessment of complex invasive fungal disease and opportunistic co-infections in patients with acute leukemia prior to allogeneic hematopoietic cell transplant.Transpl Infect Dis. 2021 Jun;23(3):e13547. doi: 10.1111/tid.13547. Epub 2020 Dec 28. Transpl Infect Dis. 2021. PMID: 33338319 Review.
-
How accurate is high-resolution computed tomography of the chest in differentiating between pulmonary invasive fungal infections and other pulmonary infections in children with cancer?Pediatr Radiol. 2025 Feb;55(2):268-279. doi: 10.1007/s00247-024-06112-2. Epub 2024 Dec 17. Pediatr Radiol. 2025. PMID: 39688678
-
Differential diagnosis of pulmonary infections in immunocompromised patients using high-resolution computed tomography.Eur Radiol. 2019 Nov;29(11):6089-6099. doi: 10.1007/s00330-019-06235-3. Epub 2019 May 6. Eur Radiol. 2019. PMID: 31062135
-
Pulmonary infections after renal transplantation: a prospective study from a tropical country.Transpl Int. 2021 Mar;34(3):525-534. doi: 10.1111/tri.13817. Epub 2021 Feb 26. Transpl Int. 2021. PMID: 33423313
-
Computed tomography-guided localization of pulmonary nodules prior to thoracoscopic surgery.Thorac Cancer. 2023 Jan;14(2):119-126. doi: 10.1111/1759-7714.14754. Epub 2022 Dec 8. Thorac Cancer. 2023. PMID: 36482812 Free PMC article. Review.
References
-
- Simpson S., Kay F.U., Abbara S., et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J Thorac Imaging. 2020;35(4):219–227. - PMC - PubMed
-
- Litmanovich D.E., Chung M., R Kirkbride R., et al. Review of chest radiograph findings of COVID-19 pneumonia and suggested reporting language. J Thorac Imaging. 2020;35(6):354–360. - PubMed
Publication types
LinkOut - more resources
Full Text Sources