

Continuity and breaches in GP care and their associations with mortality for patients with chronic disease: an observational study using Norwegian registry data
- PMID: 38621803
- PMCID: PMC11044022
- DOI: 10.3399/BJGP.2023.0211
Continuity and breaches in GP care and their associations with mortality for patients with chronic disease: an observational study using Norwegian registry data
Abstract
Background: Despite many benefits of continuity of care with a named regular GP (RGP), continuity is deteriorating in many countries.
Aim: To investigate the association between RGP continuity and mortality, in a personal list system, in addition to examining how breaches in continuity affect this association for patients with chronic diseases.
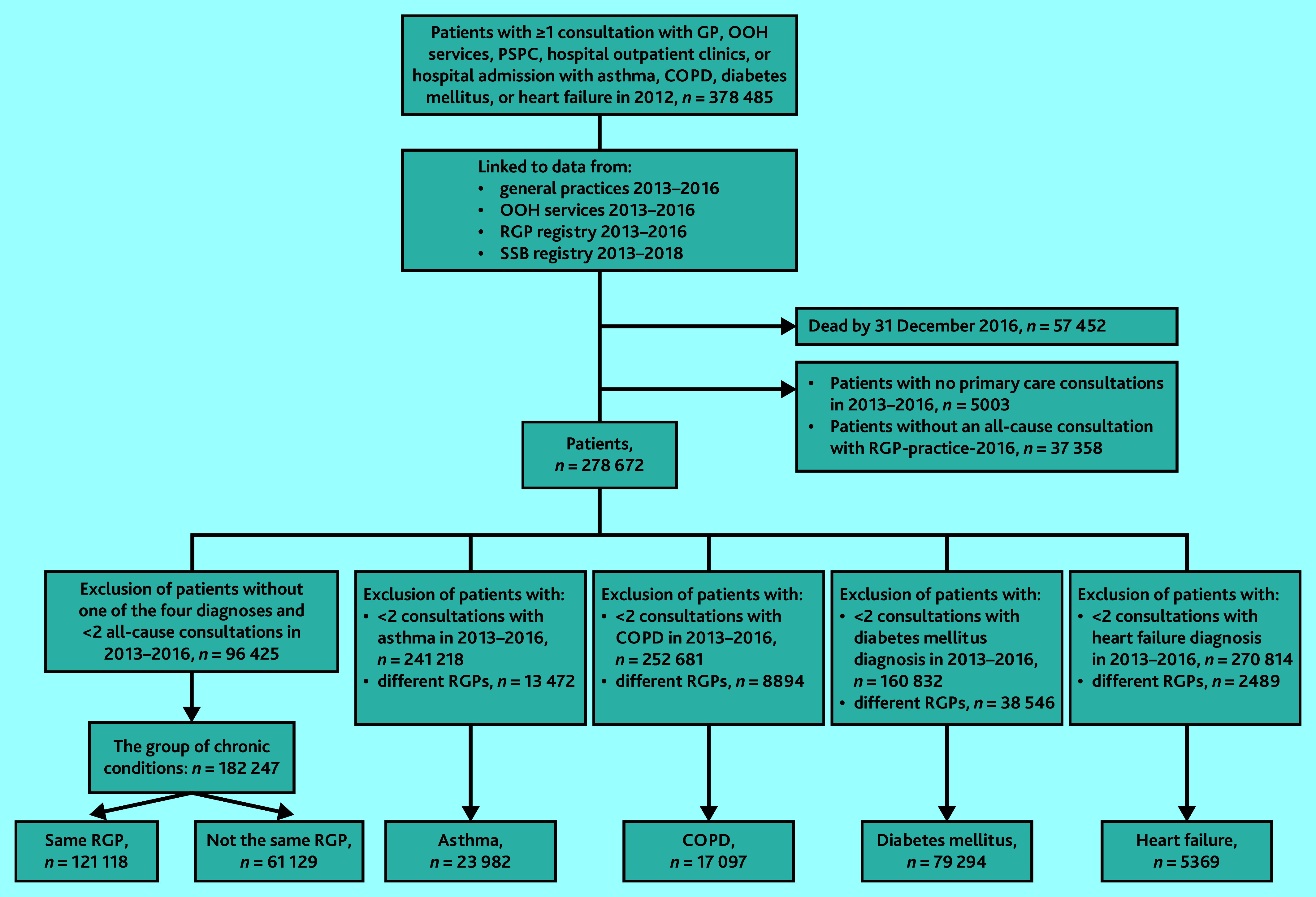
Design and setting: A registry-based observational study using Norwegian primary care consultation data for patients with asthma, chronic obstructive pulmonary disease (COPD), diabetes mellitus, or heart failure.
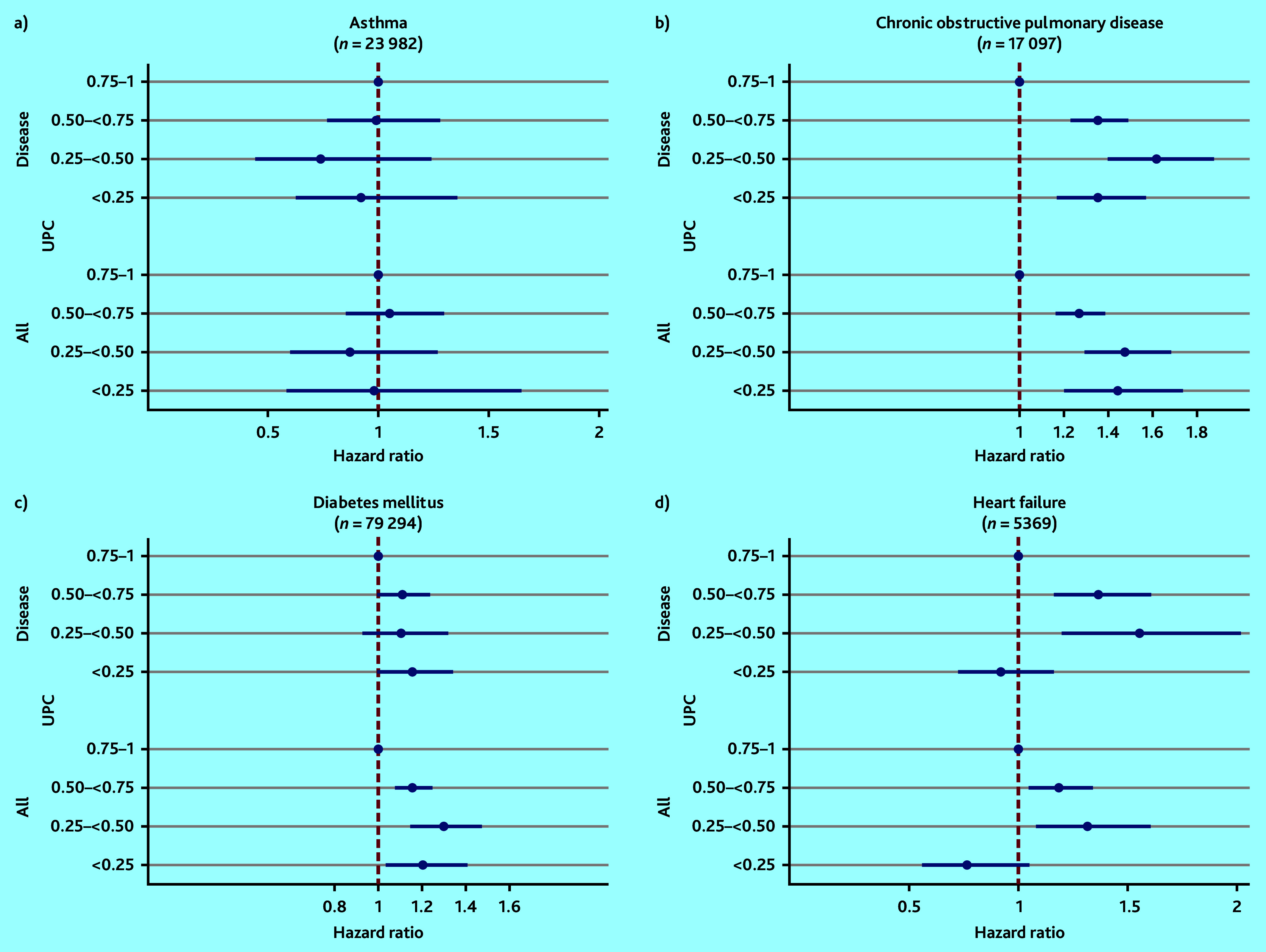
Method: The Usual Provider of Care (UPC, value 0-1) Index was used to measure both disease-related (UPCdisease) and overall (UPCall) continuity with the RGP at the time of consultation. In most analyses, patients who changed RGP during the study period were excluded. In the combined group of all four chronic conditions, the proportion of consultations with other GPs and out-of-hours services was calculated. Cox regression models calculated the associations between continuity during 2013-2016 and mortality in 2017-2018.
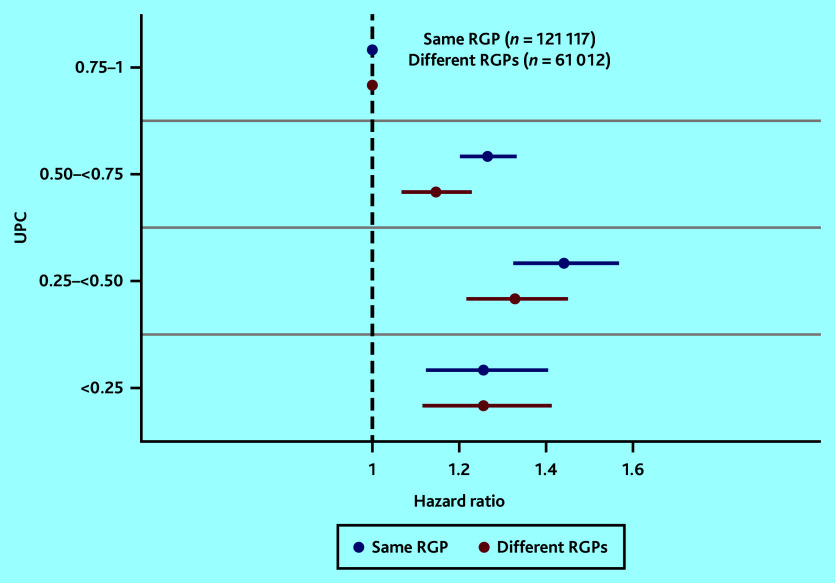
Results: Patients with COPD with UPCdisease <0.25 had 47% increased risk of dying within 2 years (hazard ratio 1.47, 95% confidence interval = 1.22 to 1.64) compared with those with UPCdisease ≥0.75. Mortality also increased with decreasing UPCdisease for patients with heart failure and decreasing UPCall for those with diabetes. In the combined group of chronic conditions, mortality increased with decreasing UPCall. This latter association was also found for patients who had changed RGP.
Conclusion: Higher disease-related and overall RGP UPC are both associated with lower mortality. However, changing RGP did not significantly affect mortality, indicating a compensatory benefit of informational and management continuity in a patient list system.
Keywords: chronic disease; continuity of care; general practice; mortality; observational study; primary health care.
© The Authors.
Conflict of interest statement
The authors have declared no competing interests.
Figures
Similar articles
-
Continuity of care for patients with chronic disease: a registry-based observational study from Norway.Fam Pract. 2022 Jul 19;39(4):570-578. doi: 10.1093/fampra/cmab107. Fam Pract. 2022. PMID: 34536072 Free PMC article.
-
Personal continuity of care in Norwegian general practice: a national cross-sectional study.Scand J Prim Health Care. 2012 Dec;30(4):214-21. doi: 10.3109/02813432.2012.735554. Epub 2012 Oct 31. Scand J Prim Health Care. 2012. PMID: 23113798 Free PMC article.
-
Continuity of care and mortality for patients with chronic disease: an observational study using Norwegian registry data.Fam Pract. 2023 Dec 22;40(5-6):698-706. doi: 10.1093/fampra/cmad025. Fam Pract. 2023. PMID: 37074143 Free PMC article.
-
Continuity of care and its effect on readmissions for COPD patients: A comparative study of Norway and Germany.Health Policy. 2018 Jul;122(7):737-745. doi: 10.1016/j.healthpol.2018.05.013. Epub 2018 May 26. Health Policy. 2018. PMID: 29933893 Review.
-
Patient involvement in the encounter between general practice and patients with a chronic disease. Results of a scoping review focusing on type 2 diabetes and obstructive pulmonary disease.Eur J Gen Pract. 2022 Dec;28(1):260-269. doi: 10.1080/13814788.2022.2153827. Eur J Gen Pract. 2022. PMID: 36503359 Free PMC article.
Cited by
-
Impact of general practitioners and specialists on mortality: a longitudinal study.BMC Health Serv Res. 2025 Jun 2;25(1):785. doi: 10.1186/s12913-025-12919-y. BMC Health Serv Res. 2025. PMID: 40457396 Free PMC article.
References
-
- VanGompel EC, Jerant AF, Franks PM. Primary care attributes associated with receipt of preventive care services: a national study. JABFM. 2015;28(6):733–741. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical