

Intention-to-treat outcomes utilising a stringent event definition in children and young people treated with tisagenlecleucel for r/r ALL through a national access scheme
- PMID: 38622139
- PMCID: PMC11018620
- DOI: 10.1038/s41408-024-01038-2
Intention-to-treat outcomes utilising a stringent event definition in children and young people treated with tisagenlecleucel for r/r ALL through a national access scheme
Abstract
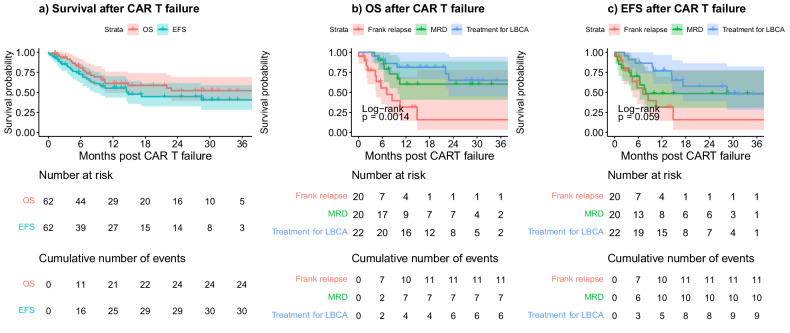
CAR T-cell therapy has transformed relapsed/refractory (r/r) B-cell precursor acute lymphoblastic leukaemia (B-ALL) management and outcomes, but following CAR T infusion, interventions are often needed. In a UK multicentre study, we retrospectively evaluated tisagenlecleucel outcomes in all eligible patients, analysing overall survival (OS) and event-free survival (EFS) with standard and stringent definitions, the latter including measurable residual disease (MRD) emergence and further anti-leukaemic therapy. Both intention-to-treat and infused cohorts were considered. We collected data on feasibility of delivery, manufacture, toxicity, cause of therapy failure and followed patients until death from any cause. Of 142 eligible patients, 125 received tisagenlecleucel, 115/125 (92%) achieved complete remission (CR/CRi). Severe cytokine release syndrome and neurotoxicity occurred in 16/123 (13%) and 10/123 (8.1%), procedural mortality was 3/126 (2.4%). The 2-year intent to treat OS and EFS were 65.2% (95%CI 57.2-74.2%) and 46.5% (95%CI 37.6-57.6%), 2-year intent to treat stringent EFS was 35.6% (95%CI 28.1-44.9%). Median OS was not reached. Sixty-two responding patients experienced CAR T failure by the stringent event definition. Post failure, 1-year OS and standard EFS were 61.2% (95%CI 49.3-75.8) and 55.3% (95%CI 43.6-70.2). Investigation of CAR T-cell therapy for B-ALL delivered on a country-wide basis, including following patients beyond therapy failure, provides clinicians with robust outcome measures. Previously, outcomes post CAR T-cell therapy failure were under-reported. Our data show that patients can be successfully salvaged in this context with good short-term survival.
© 2024. The Author(s).
Conflict of interest statement
SG, SB, BU and DM have received honoraria from Novartis. MO’R has received honoraria/support to attend conferences from Novartis. CR is on advisory board and receives honoraria from Novartis. AC receives consulting fees from Novartis. EN is on advisory board and has received support to attend conferences from Novartis. The rest of authors have no competing interests in relation to this work.
Figures




References
-
- Laetsch TW, Maude SL, Rives S, Hiramatsu H, Bittencourt H, Bader P, et al. Three-year update of tisagenlecleucel in pediatric and young adult patients with relapsed/refractory acute lymphoblastic leukemia in the ELIANA trial. J Clin Oncol. 2023;41:1664–9. doi: 10.1200/JCO.22.00642. - DOI - PMC - PubMed
-
- Myers RM, Jacoby E, Pulsipher MA, Pasquini MC, Grupp SA, Shah NN, et al. Clinical variables associated with improved outcomes for children and young adults treated with chimeric antigen receptor T cells for B cell acute lymphoblastic leukemia: a decade of chimeric antigen receptor translation. Transpl Cell Ther. 2023;29:598–607. doi: 10.1016/j.jtct.2023.07.016. - DOI - PMC - PubMed
